Pain during your periods shouldn’t feel normal. Heavy bleeding that disrupts your daily life isn’t something you should accept. Yet thousands of women live with these symptoms, believing surgery is their only option. The truth? You can learn how to get rid of fibroids without surgery through proven alternatives that work.
Many women diagnosed with uterine fibroids fear they’ll need a hysterectomy. That’s understandable—but outdated. Modern medicine offers effective treatments that don’t require removing your uterus or going under the knife for major surgical procedures.

Can Fibroids Be Cured Permanently Without Surgery?
This question troubles many women facing a fibroid diagnosis. While fibroids are benign tumors that grow in the uterine muscle, the idea of “cure” needs clarification.
Fibroids don’t work like infections you can completely eliminate. However, non-surgical treatments can shrink them significantly, relieve your symptoms, and prevent new ones from causing problems. Think of it as managing the condition rather than chasing an absolute cure.
What actually works for permanent relief?
- Uterine artery embolization blocks blood flow to fibroids, causing them to shrink
- Focused ultrasound targets and destroys fibroid tissue
- Hormonal treatments can manage growth in some cases
- Natural approaches may help smaller, non-symptomatic fibroids
The key is finding what works for your specific situation—the size of your fibroids, their location, your symptoms, and your future plans matter.
How to Get Rid of Fibroids Without Surgery
Getting rid of fibroids without going through major surgery is more achievable than most people realize. The medical field has developed several minimally invasive procedures that offer real results.
Uterine Artery Embolization (UAE)
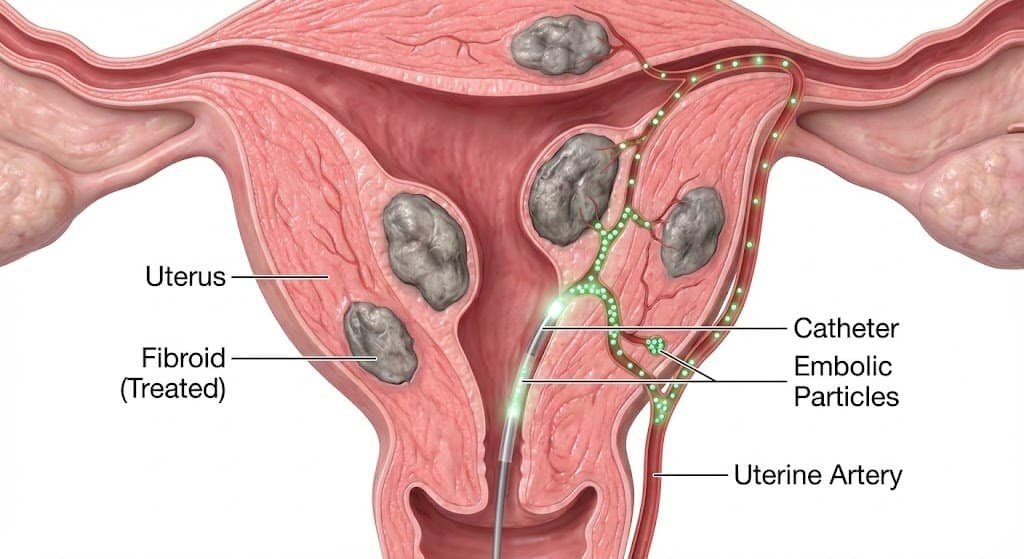
This procedure has changed everything for women seeking alternatives to hysterectomy. During UAE, a specialist injects tiny particles into the arteries feeding your fibroids. Without blood supply, these tumors shrink naturally over the following months.
The benefits are remarkable:
- Done through a small catheter—no large incisions
- You keep your uterus intact
- Recovery takes days, not weeks
- Over 90% of women experience symptom relief
- Pregnancy remains possible for many women
Focused Ultrasound Treatment
High-intensity focused ultrasound waves target fibroid tissue without cutting. It’s completely non-invasive, though it works best for certain types and locations of fibroids.
Medication Options
Gonadotropin-releasing hormone agonists can temporarily shrink fibroids by lowering hormone levels. While not permanent, they offer relief and can help you avoid surgical intervention while planning your next steps.
How to Shrink Fibroids Naturally Without Surgery
Natural approaches won’t replace medical treatment for symptomatic fibroids, but they can help manage smaller ones and support your overall health.
Lifestyle Changes That Matter
Your daily habits affect fibroid growth more than you might think. Women who maintain a healthy weight often experience fewer symptoms. Regular exercise helps balance hormones and reduce inflammation.
Stress Management
Chronic stress elevates cortisol, which can influence fibroid development. Finding ways to relax—whether through meditation, yoga, or simply taking breaks—supports your body’s natural balance.
Natural Supplements
Some people find relief using:
- Green tea extract
- Vitamin D supplementation
- Curcumin (found in turmeric)
- Fish oil for anti-inflammatory benefits
Always discuss supplements with your doctor before starting, especially if you’re taking other medicine or planning pregnancy.
Fibroid Removal Without Surgery
When people talk about “fibroid removal,” they usually imagine surgical procedures. But several minimally invasive options exist that don’t require traditional surgery.
Uterine Fibroid Embolization (UFE)
This procedure, offered by interventional radiology specialists like Dr. Samir Abdel Ghaffar, removes the fibroid’s blood supply rather than cutting it out. The result? Fibroids shrink and symptoms disappear without the risks of major surgery.
The procedure takes about an hour. You’ll have a small incision in your groin or wrist where the catheter enters. Most women go home the same day.
What Makes UFE Different?
Unlike surgical removal, UFE:
- Treats all fibroids at once, regardless of number
- Preserves the uterus completely
- Requires no general anesthesia in most cases
- Offers faster recovery than traditional options
- Reduces risk of fibroid recurrence
Best Treatment for Fibroids
The “best” treatment depends entirely on your situation. What works beautifully for one woman might not suit another.
Factors Your Doctor Should Consider:
- Size and location of your fibroids
- Severity of symptoms you’re experiencing
- Your age and whether you want future pregnancy
- Overall health conditions
- Personal preferences about treatment approach
Comparing Your Options
For symptomatic fibroids causing heavy bleeding and pain, uterine artery embolization often emerges as the most effective treatment. It balances efficacy with minimal invasion, offering relief without the recovery time of abdominal hysterectomy.
Hysterectomy removes the uterus entirely—a definitive solution, but one that ends fertility and requires major surgery. Many women who choose hysterectomy later discover they could have preserved their uterus through alternatives.
Myomectomy removes individual fibroids while keeping the uterus. It requires surgical incisions and fibroids can return, but some women prefer this approach.
Fibroid Removal Without Surgery Cost
Treatment costs vary significantly based on location, procedure type, and insurance coverage.
Understanding the Financial Picture
Non-surgical fibroid removal options like UFE typically cost less than traditional surgery when you factor in:
- Shorter hospital stays (often same-day discharge)
- Faster return to work
- Lower complication rates
- No need for extended recovery care
Many insurance plans cover uterine fibroid embolization, recognizing it as an effective alternative to surgical procedures. Check with your provider about specific coverage.
For consultations with Dr. Samir Abdel Ghaffar regarding treatment options and costs:
In London, UK:
- Clinic: 00442081442266
- WhatsApp: 00447377790644
In Cairo, Egypt:
- Booking: +201000881336
- WhatsApp: +201000881336
How to Remove Fibroid Naturally at Home 🌿
Complete fibroid removal at home isn’t realistic—these are physical tumors growing in your uterine muscle. However, you can manage symptoms and potentially slow growth through home-based approaches.
Daily Habits That Help:
Start your day with anti-inflammatory foods. Add ginger to your morning tea. Choose whole grains over processed options. These small changes support hormonal balance.
Heat Therapy
A heating pad on your lower abdomen can relieve cramps and pelvic discomfort during periods. While it doesn’t remove fibroids, it manages the pain they cause.
Herbal Support
Some women find relief using:
- Chasteberry (may help balance hormones)
- Milk thistle (supports liver function and hormone metabolism)
- Dandelion root (aids detoxification)
Remember: natural doesn’t mean risk-free. Discuss any herbal remedies with your healthcare provider.
Treatment of Fibroid Without Surgery
Modern treatment of fibroid without surgery centers on minimally invasive procedures that target the root problem.
Uterine Artery Embolization: The Gold Standard 💫
Dr. Samir Abdel Ghaffar specializes in this procedure, offering women a proven alternative to hysterectomy. As a consultant in interventional radiology, he performs UAE using advanced catheterization techniques.
The Procedure Process:
You’ll receive local anesthesia and mild sedation. A tiny tube goes into an artery in your wrist or groin. Using X-ray guidance, the doctor navigates to the arteries feeding your fibroids and injects small particles that block blood flow.
Without their blood supply, fibroids begin shrinking within weeks. Most women notice symptom improvement within the first month, with maximum results appearing over three to six months.
Recovery Reality:
- Most women rest for a few days
- Return to normal activities within a week
- Avoid heavy lifting for two weeks
- Full recovery typically takes one month
Compare this to surgical options requiring six to eight weeks of recovery.
7 Foods for Shrinking Fibroids
While food alone won’t eliminate fibroids, certain dietary choices support your body in managing them.
1. Leafy Greens
Spinach, kale, and collard greens provide iron (important if you have heavy bleeding) and support liver function for hormone balance.
2. Fatty Fish
Salmon, mackerel, and sardines offer omega-3 fatty acids that reduce inflammation and may slow fibroid growth.
3. Whole Grains
Brown rice, quinoa, and oats provide fiber that helps your body eliminate excess hormones. They also stabilize blood sugar, which affects hormone production.
4. Legumes
Beans and lentils offer plant-based protein and fiber. They’re filling, nutritious, and support hormone balance.
5. Cruciferous Vegetables
Broccoli, cauliflower, and Brussels sprouts contain compounds that help your body metabolize estrogen more effectively.
6. Berries 🫐
Blueberries, strawberries, and raspberries provide antioxidants that fight inflammation and support overall health.
7. Green Tea
Rich in EGCG, a compound that may inhibit fibroid growth. Aim for two to three cups daily.
Foods to Limit:
- Red meat (linked to increased fibroid risk)
- Processed foods high in added sugars
- Alcohol (affects hormone metabolism)
- High-fat dairy products
Understanding Your Treatment Options
Choosing how to proceed with fibroid treatment affects your health, fertility, and quality of life. Understanding all available options empowers better decisions.
Minimally Invasive Procedures
These treatments offer middle ground between doing nothing and major surgery. They include:
- Uterine Fibroid Embolization (UFE): Blocks blood supply to fibroids through catheterization. Highly effective for most women regardless of fibroid size or number.
- MRI-Guided Focused Ultrasound: Uses ultrasound waves to destroy fibroid tissue. Works best for fibroids in certain locations within the uterus.
- Radiofrequency Ablation: Destroys fibroid tissue using heat energy. Requires small incisions but isn’t technically major surgery.
When Surgery Becomes Necessary
Some situations genuinely require surgical intervention:
- Fibroids causing severe anemia despite treatment
- Rapid growth requiring tissue diagnosis
- Fibroids affecting other organs
- Failure of minimally invasive treatments
Even then, myomectomy (removing just the fibroids) often works better than hysterectomy for women wanting to preserve fertility.
Frequently Asked Questions
How can I naturally break down my fibroids?
Your body can’t completely break down fibroids naturally, but lifestyle changes help manage them. Focus on anti-inflammatory foods, maintain healthy weight, exercise regularly, and manage stress. These approaches support hormonal balance and may slow growth. For actual shrinkage, you’ll need medical treatment like UAE.
What pills shrink fibroids?
Gonadotropin-releasing hormone agonists temporarily shrink fibroids by reducing estrogen. Birth control pills don’t shrink fibroids but can manage heavy bleeding. Tranexamic acid reduces bleeding during periods. Anti-prostaglandin medications relieve pain and cramps. Your doctor will recommend the best medicine based on your symptoms.
What makes fibroids stop growing?
Fibroids grow in response to hormones, particularly estrogen and progesterone. They typically stop growing during menopause when hormone levels drop. Treatments like GnRH agonists create temporary menopause-like conditions. UAE cuts off blood supply, causing fibroids to shrink and stop growing. Maintaining healthy hormone balance through lifestyle may slow growth.
What to drink to flush out fibroids?
No drink can “flush out” fibroids—they’re solid tumors in your uterine muscle. However, green tea contains compounds that may inhibit fibroid growth. Water helps your body function optimally. Avoid alcohol, which can affect hormone metabolism. Focus on medical treatments that actually shrink fibroids rather than seeking miracle drinks.
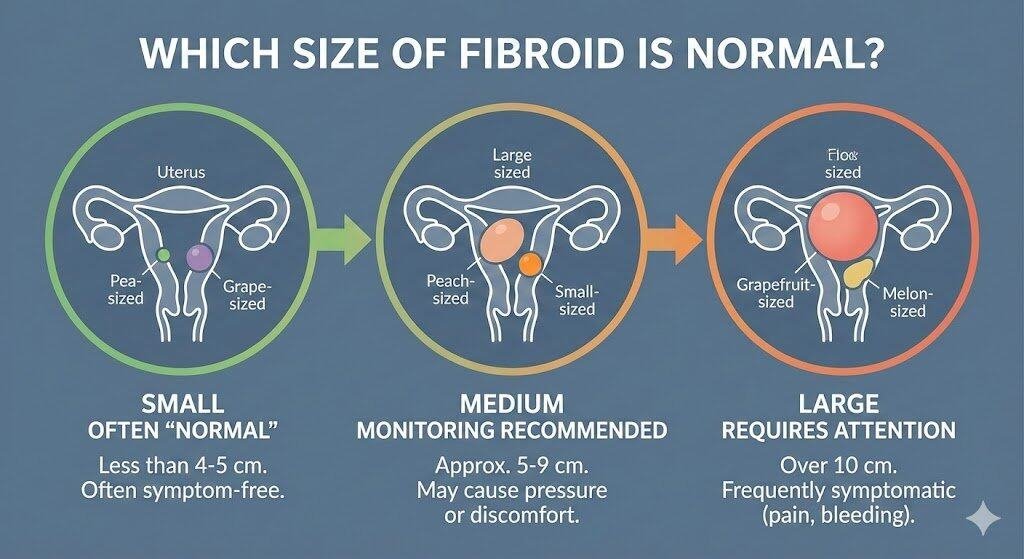
What size fibroids need surgery?
Size alone doesn’t determine whether you need surgery. A large fibroid causing no symptoms might not require treatment, while a small one pressing on your bladder could need intervention. Generally, fibroids over 10 cm often require treatment. However, your symptoms, fibroid location, and future pregnancy plans matter more than size alone. Many women with large fibroids benefit from UAE rather than surgery.
Which food can remove fibroids?
No food removes fibroids. However, certain foods support fibroid management: leafy greens provide nutrients and support hormone balance; fatty fish offers anti-inflammatory omega-3s; cruciferous vegetables help metabolize estrogen; legumes provide fiber for hormone elimination; berries fight inflammation. These foods complement medical treatment but don’t replace it.
What happens if I don’t remove my fibroids?
Small, non-symptomatic fibroids often require no treatment. Many women live normally with fibroids. However, symptomatic fibroids can cause heavy bleeding leading to anemia, severe pelvic pain affecting daily life, frequent urination from bladder pressure, constipation from pressure on intestines, and potential pregnancy complications. Treatment prevents these issues and improves quality of life.
What are the main causes of fibroids?
Doctors don’t know exactly what causes fibroids, but several factors contribute: hormones (estrogen and progesterone) promote fibroid growth, genetic factors play a role, early menstruation increases risk, family history matters significantly, obesity and diet affect risk, and vitamin D deficiency shows correlation. Most women develop some fibroids during reproductive years.
Which vitamin shrinks fibroids?
Vitamin D shows promise in fibroid management. Studies suggest women with adequate vitamin D levels have lower fibroid risk. Supplementation may slow growth but won’t dramatically shrink existing fibroids. Always consult your doctor about appropriate dosing. Other nutrients like B vitamins support hormone metabolism. However, vitamins work best as part of comprehensive treatment, not standalone solutions.
Taking Control of Your Fibroid Treatment
Living with symptomatic fibroids affects every aspect of your life—from missing work due to heavy periods to avoiding activities because of pain. You don’t have to accept this as normal, and you definitely don’t need to lose your uterus to find relief.
Uterine artery embolization offers a middle path. It’s effective enough to eliminate symptoms yet gentle enough to preserve your fertility and avoid major surgery. Women who choose UAE typically experience dramatic improvement in their quality of life without the risks and recovery time of traditional surgery.
Dr. Samir Abdel Ghaffar has helped countless women discover this alternative. As a consultant in interventional radiology with extensive experience in catheterization techniques, he provides expert care for fibroid treatment without surgery.
Your next steps:
- Schedule a consultation to discuss your specific situation
- Learn about UFE and whether it’s right for you
- Understand recovery expectations and timeline
- Make an informed decision about your health
Contact Dr. Samir Abdel Ghaffar:
London, UK:
- Clinic: 00442081442266
- WhatsApp: 00447377790644
Cairo, Egypt:
- Booking: +201000881336
- WhatsApp: +201000881336
Don’t let fibroids control your life. Effective treatment exists that respects your body, preserves your options, and gets you back to living fully. The alternative to hysterectomy you’ve been searching for is here—and it works.