تشعرين بألم شديد وقت الدورة الشهرية؟ تعانين من نزيف غزير يؤثر على حياتك اليومية؟ ربما سمعتِ من طبيبك أن علاج الأورام الليفية بدون استئصال الرحم خيار غير ممكن، لكن هذا ليس صحيحاً تماماً. الحقيقة أن الطب التداخلي الحديث طور طرقاً فعالة تحافظ على رحمك بينما تتخلصين من الأورام وأعراضها. في هذا المقال، سنكتشف معاً كيف تستطيعين الاستفادة من أحدث التقنيات الطبية التي غيرت حياة آلاف النساء، وكيف يمكنك اتخاذ القرار الصحيح لصحتك.
Table of Contents
هل يمكن علاج الأورام الليفية بدون استئصال الرحم؟ – نسبة نجاح 95%
نعم، بكل تأكيد. وهذا ما تثبته الدراسات الطبية والتجارب السريرية لآلاف النساء حول العالم.
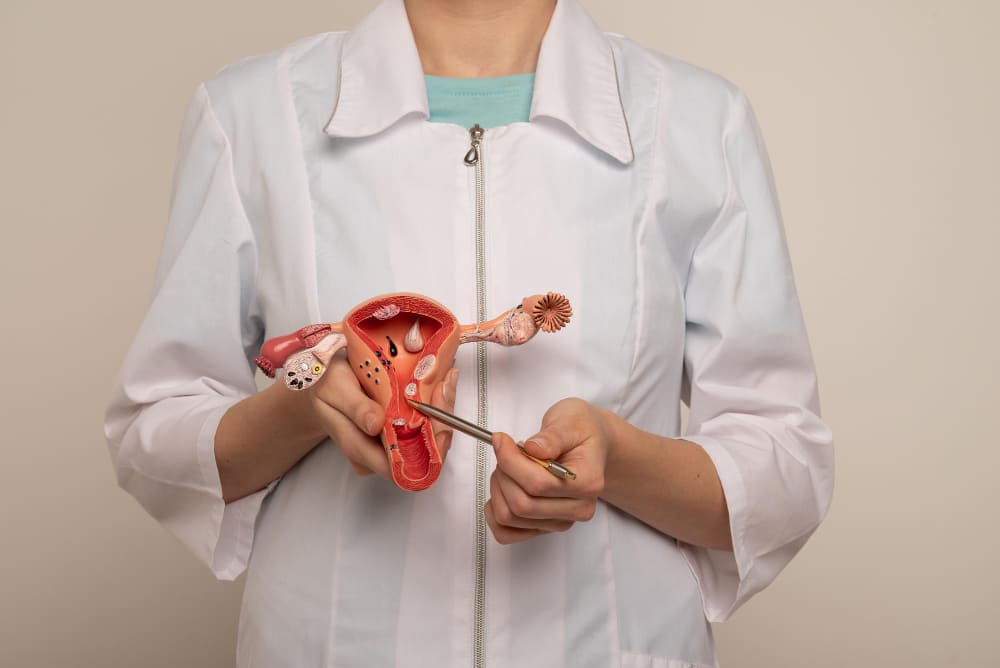
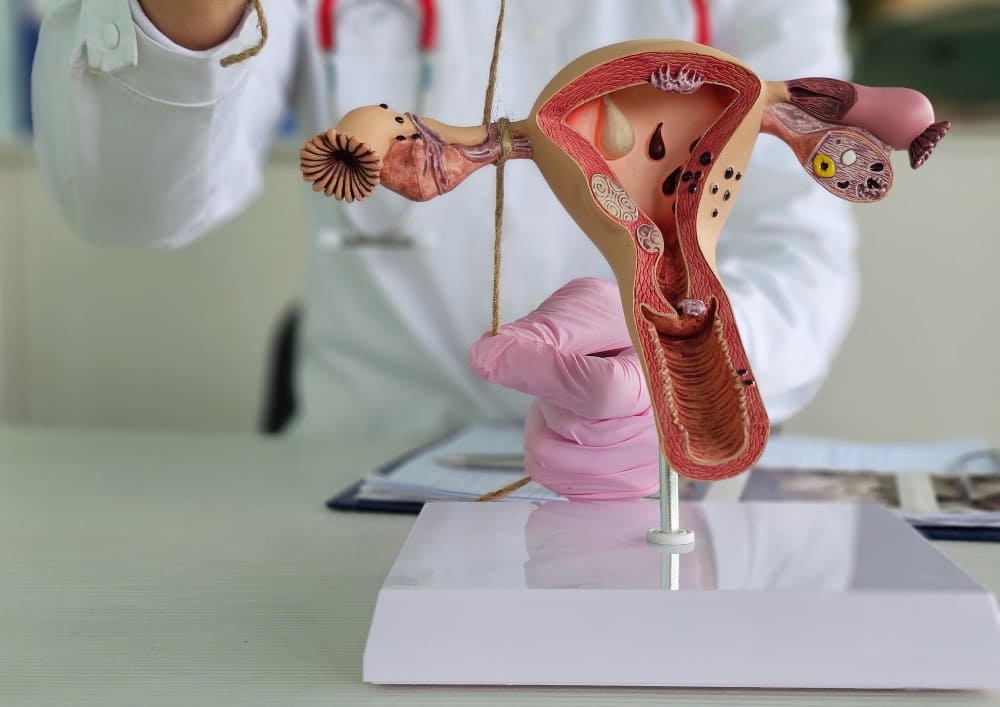
الأورام الليفية الرحمية (Uterine Fibroids) أورام حميدة تنمو في جدران الرحم. المهم أنها حميدة وليست سرطانية، مما يعني أن هناك خيارات عديدة للتعامل معها. ليس كل ورم يتطلب إزالة الرحم بالكامل.
دكتور سمير عبد الغفار، استشاري الأشعة التداخلية، يقدم حلولاً متعددة لعلاج الورم الليفي دون اللجوء للجراحة التقليدية. من أشهر هذه الطرق:
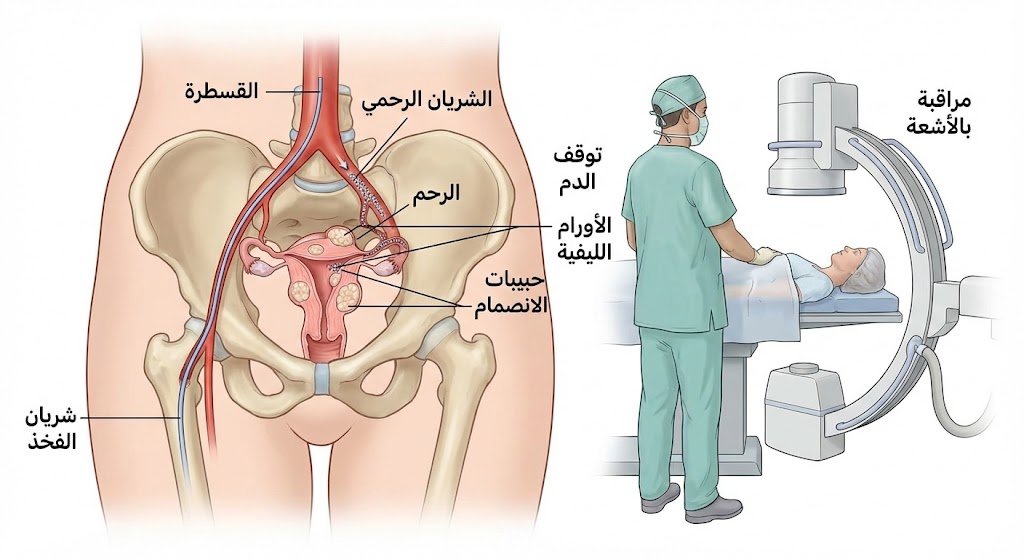
علاج الأورام الليفية بدون جراحة يعتمد على مبدأ بسيط لكن ذكي جداً: قطع التروية الدموية عن الورم.
كل ورم ليفي يحتاج إلى شرايين لتغذيه، تماماً كأي خلية حية. عندما نقطع هذا الدم عن طريق القسطرة الموجهة بالأشعة، الورم يبدأ بالانكماش والاختفاء تدريجياً.
خطوات الإجراء:
التقييم الأولي: فحص بالموجات الصوتية أو الرنين المغناطيسي لتحديد موقع وحجم الأورام
إدخال القسطرة: عبر شريان الفخذ (أكبر شرايين الجسم)
توجيه دقيق: باستخدام الأشعة السينية الحية
حقن الجزيئات: مواد خاصة تقطع الدم عن الورم
المراقبة: التأكد من نجاح الإجراء
كل هذا بدون جراحة – لا شقوق جراحية، لا مخاطر التخدير العام، ولا فترة تعافي طويلة.
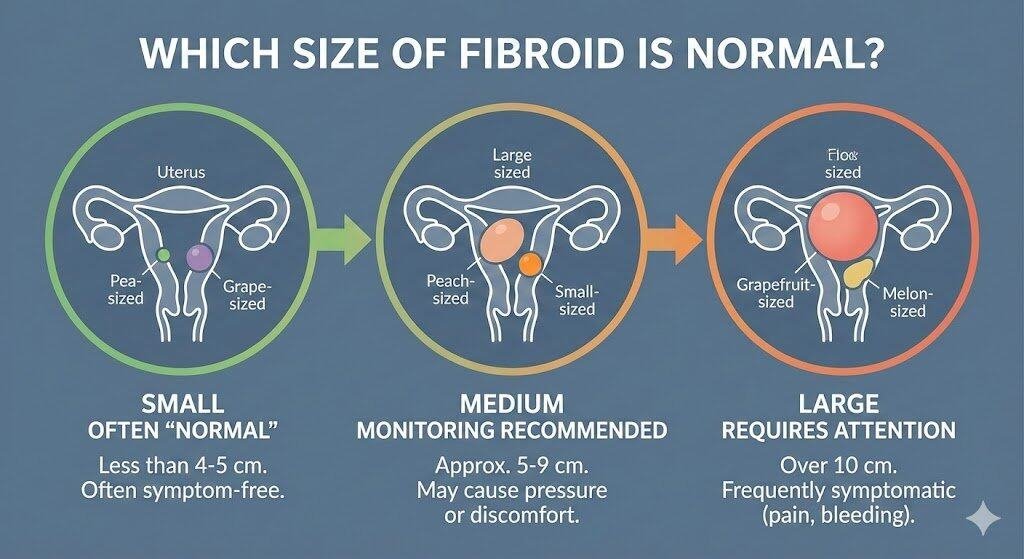
حجم الورم الليفي ليس دائماً مؤشراً على الخطورة. بعض النساء لديهن أورام صغيرة لكن أعراضها حادة جداً، وأخريات لديهن أورام كبيرة لكن بدون أعراض تذكر.
لكن هناك حالات تتطلب تدخلاً سريعاً:
الأورام الكبيرة جداً (أكثر من 10 سم): قد تضغط على المثانة أو الأمعاء
النزيف الغزير: الذي يسبب فقر دم شديد
الألم الحاد: الذي يؤثر على نوعية الحياة
تأثر الخصوبة: عندما يؤثر الورم على فرص الحمل
ضغط على الأعصاب أو الأوعية الدموية: قد يسبب مضاعفات خطيرة
إذا كنتِ تعانين من أي من هذه الحالات، استشارة دكتور سمير عبد الغفار استشاري الأشعة التداخلية أمر حتمي. لكن الخبر السار أن معظم هذه الحالات يمكن علاجها بدون استئصال الرحم.
الكثيرات يسألن: “هل فعلاً هذا العلاج يعمل؟” والإجابة تأتي من تجارب النساء اللواتي خضعن للعلاج.
ملخص التجارب:
ريم من القاهرة: كانت تعاني من ورم ليفي بحجم 8 سم مع نزيف غزير جداً. عملت قسطرة رحم مع د. سمير، والآن (بعد 6 أشهر) انكمش الورم إلى 3 سم والدورة أصبحت طبيعية جداً.
لينا من الإسكندرية: كانت مخيفة جداً من العملية الجراحية. بعد استشارة د. سمير، اختارت قسطرة الرحم. تقول: “ما كان ألم على الإطلاق، والتعافي كان أسهل بكثير مما توقعت.”
هنا من لندن: كانت تخطط للحمل لكن الأورام الليفية كانت تعيقها. بعد العلاج بقسطرة الرحم، حملت بشكل طبيعي بعد 8 أشهر.
هذه القصص ليست استثناءات – آلاف النساء حول العالم لديهن قصص مشابهة.
علاج الورم الليفي بالأعشاب: الحقيقة والخيال
أولاً، دعيني أكون صريحة معك: لا توجد أعشاب يمكنها إزالة الورم الليفي بالكامل.
لكن هناك أعشاب قد تساعد على تقليل الأعراض:
الزنجبيل: مضاد التهاب قوي، قد يساعد على تقليل الألم
الكركم: يحتوي على الكركمين الذي له خصائص مضادة للالتهاب
شاي الأعشاب الخاص: مثل شاي القرفة قد يساعد على تنظيم الدورة
فيتامين د: نقصه مرتبط بنمو الأورام الليفية
لكن:
الأعشاب وحدها لن توقف نمو الورم، ولن تقضي على الأعراض الحادة. للحصول على علاج فعال للأورام الليفية الرحمية، تحتاجين إلى تدخل طبي فعلي.
الأعشاب قد تكون مساعدة مكملة فقط، مع الرعاية الطبية المناسبة.
الورم الليفي في الرحم والجماع: ماذا تتوقعين
سؤال حساس لكن مهم جداً: كيف يؤثر الورم الليفي على العلاقة الجنسية؟
الحقيقة: معظم الأورام الليفية الصغيرة والمتوسطة لا تؤثر على العملية الجنسية نفسها.
لكن قد تشعرين بـ:
ألم أثناء أو بعد الجماع: خاصة إذا كان الورم قريب من عنق الرحم
نزيف بعد الجماع: قد يحدث في بعض الحالات
فقدان الرغبة الجنسية: بسبب الألم والأعراض الأخرى
الخبر الجيد:
بعد علاج الأورام الليفية بنجاح، معظم النساء يلاحظن تحسناً كبيراً في حياتهن الجنسية. عندما تختفي الأعراض، تعود الحياة إلى طبيعتها.
تجربتي في علاج الورم الليفي في الرحم: رحلة التعافي
تجارب النساء الفعلية تخبرنا الكثير:
اليوم الأول بعد العملية:
شعور بخفة خفيفة في البطن
تقلصات خفيفة جداً (أقل من تقلصات الدورة الشهرية)
إمكانية المشي والحركة الطبيعية
الأسبوع الأول:
عودة الطاقة تدريجياً
إمكانية العودة للعمل
اختفاء معظم الألم
الشهر الأول:
تحسن واضح في الأعراض
الدورة الشهرية قد تكون خفيفة أكثر
بعد 3-6 أشهر:
اختفاء النزيف الغزير
انكماش الأورام بشكل ملحوظ
عودة الحياة إلى طبيعتها تماماً
هذا بعكس الجراحة التقليدية التي قد تحتاج 4-6 أسابيع للتعافي وقد تترك ندبات.
الخيارات الطبية الحديثة: ما وراء الجراحة
لديك الآن خيارات متعددة لعلاج الأورام الليفية أكثر من أي وقت مضى:
د. سمير عبد الغفار يساعدك على اختيار الخيار الأنسب لحالتك.
الأعراض التي تنتظري تحسنها بعد العلاج
بعد علاج الأورام الليفية بدون استئصال الرحم بنجاح، تتوقعين:
✓ تقليل النزيف: 80-90% من النساء يلاحظن تقليص النزيف بشكل كبير ✓ تقليل الألم: معظم الآلام تختفي تماماً ✓ تحسن الدورة الشهرية: أصبحت منتظمة وأقل ألماً ✓ زيادة الطاقة: بسبب تحسن فقر الدم ✓ تحسن الخصوبة: فرص الحمل تزداد ✓ نوعية حياة أفضل: بشكل عام وملحوظ
لماذا تختارين د. سمير عبد الغفار – استشاري الأشعة التداخلية
خبرة واسعة: تعامل مع مئات الحالات من الأورام الليفية والأورام الأخرى
عيادات في لندن والقاهرة: يعني إمكانية الوصول من أي مكان
تقنيات حديثة: يستخدم أحدث معدات الأشعة والقسطرة
نسبة نجاح عالية: موثقة وموثوقة
الأسئلة الشائعة – FAQ
كيف أصغر حجم الورم الليفي؟
تصغير حجم الورم يحتاج إلى تدخل طبي فعلي. الخيارات:
القسطرة التداخلية: تقطع الدم عن الورم فينكمش بنسبة 50-60% في الأشهر الأولى
الأدوية الهرمونية: قد تبطئ النمو لكن لا تقلل الحجم بشكل كبير
الانتظار بدون علاج: قد يبقى الورم بنفس الحجم أو ينمو مع الوقت
لا توجد طريقة طبيعية سريعة لتصغير الورم. العلاج الطبي هو الحل الفعال.
كيف أتخلص من الورم الليفي في الرحم؟
الحل الأفضل:
استشارة طبيب متخصص أولاً (مثل د. سمير) لتقييم حالتك. ثم:
إذا كان الورم صغيراً بدون أعراض: المراقبة الدورية
إذا كان الورم كبيراً أو له أعراض: قسطرة الرحم هي الخيار الأول
إذا كان هناك موانع للقسطرة: خيارات جراحية أخرى
القسطرة التداخلية هي الحل الذي تختاره معظم النساء الآن بدلاً من الجراحة.
ما هو دور فيتامين د في الأورام الليفية الرحمية؟
دور فيتامين د مهم جداً:
نقص فيتامين د مرتبط بـ:
زيادة نمو الأورام الليفية
زيادة الأعراض والألم
قلة فرص الحمل
الحل:
فحص مستويات فيتامين د (يجب أن تكون أكثر من 30 NG/ML)
إذا كانت ناقصة، تناول مكملات فيتامين د
التعرض للشمس بانتظام
تناول الأطعمة الغنية به (الأسماك، الحليب المدعم)
لكن تجدر الإشارة: فيتامين د وحده لن يزيل الورم. هو عامل مساعد فقط.
متى يتم استئصال الرحم بسبب الورم الليفي؟
استئصال الرحم يكون خياراً أخيراً في الحالات النادجة جداً:
فشل جميع العلاجات الأخرى
أورام ضخمة جداً تسبب مضاعفات خطيرة
سرطان الرحم (وهذا نادر جداً مع الأورام الليفية الحميدة)
رغبة المريضة الواضحة بعد استيعاب جميع الخيارات
الحقيقة: مع التطور الطبي الحديث، استئصال الرحم أصبح نادر جداً حالياً. معظم الحالات يمكن علاجها بدون استئصال الرحم.
ما هي الفيتامينات التي تساعد على تقليص حجم الورم الليفي؟
الفيتامينات المساعدة:
فيتامين د: كما ذكرنا، مهم جداً
فيتامين E: مضاد أكسدة قوي، قد يقلل الالتهاب
فيتامين B6: يساعد على تنظيم الهرمونات
فيتامين C: يقوي المناعة ويقلل الالتهاب
لكن:
هذه الفيتامينات تساعد على تحسين الأعراض وتبطيء النمو، لكن لا تزيل الورم. للتخلص الفعلي من الورم، تحتاجين إلى تدخل طبي (قسطرة أو جراحة).
كم يبلغ وزن الورم الليفي الذي يبلغ قطره 7 سم؟
الإجابة:
وزن الورم يختلف حسب:
نوع الورم: بعضها أكثف من بعض
موقعه: تحت الغشاء المخاطي أم داخل جدار الرحم
محتواه: بعضها يحتوي على نسيج ليفي أكثر
تقريباً: ورم قطره 7 سم يزن حوالي 100-200 غرام، لكن هذا تقريب فقط.
المهم: حجم الورم ووزنه أقل أهمية من الأعراض التي يسببها. ورم صغير قد يسبب أعراضاً حادة، وورم كبير قد لا يسبب شيء.
معلومات التواصل – ابدئي رحلة التعافي اليوم
إذا كنتِ تعانين من أعراض الأورام الليفية، فريق د. سمير عبد الغفار هنا للمساعدة. بدون جراحة، بدون ألم، بدون استئصال الرحم.
في لندن – المملكة المتحدة:
📞 رقم العيادة: 00442081442266 💬 WhatsApp: 00447377790644
في القاهرة – مصر:
📞 رقم حجز القاهرة: 00201000881336 💬 WhatsApp: 00201000881336
الخلاصة النهائية
علاج الأورام الليفية بدون استئصال الرحم لم يعد حلماً. إنه واقع يعيشه آلاف النساء اليوم.
مع قسطرة الرحم والتقنيات التداخلية الحديثة، يمكنك:
✓ الحفاظ على رحمك بالكامل ✓ تقليل الأعراض بنسبة 80-90% ✓ البقاء قادرة على الحمل الطبيعي ✓ التعافي السريع (أيام وليس أسابيع) ✓ نسبة نجاح 95%
أنتِ لا تحتاجين إلى الاستسلام للجراحة. اختاري الطريق الأفضل لصحتك.
استشارة مع د. سمير عبد الغفار الآن قد تغير حياتك للأفضل.
هذا المقال يقدم معلومات طبية عامة ولا يحل محل الاستشارة الطبية المباشرة. كل حالة فريدة وتحتاج إلى تقييم شخصي. استشيري طبيبك دائماً قبل اتخاذ أي قرار طبي.
هل تعانين من آلام الدورة الشهرية الحادة والنزيف الغزير؟ قد تكونين تعانين من الأورام الليفية، وهي حالة شائعة تؤثر على ملايين النساء حول العالم. الخبر الجيد أن الحل الذي طالما بحثتِ عنه موجود بالفعل. قسطرة الرحم للأورام الليفية تمثل ثورة حقيقية في عالم العلاج التداخلي، حيث توفر بديلاً آمناً وفعالاً عن الجراحة التقليدية. هذا الإجراء الطبي الحديث يتم إجراؤه بدون جراحة، مما يعني تعافي أسرع وآثار جانبية أقل بكثير. تابعي معنا لاكتشاف كيف يمكن لهذه التقنية المتقدمة أن تحسّن حياتك.
قسطرة الرحم للأورام الليفية (Uterine Fibroid Embolization – UFE) هي تقنية طبية تداخلية حديثة تستخدم لعلاج الأورام الليفية الرحمية بدون الحاجة إلى إجراء جراحة تقليدية. يتم في هذا الإجراء إدخال قسطرة رفيعة جداً عبر الشريان الفخذي، ثم يتم توجيهها بدقة نحو الشرايين المغذية للأورام الليفية.
الفكرة الأساسية بسيطة لكن ذكية: قطع التروية الدموية عن الورم يؤدي إلى انكماشه تدريجياً واختفاء الأعراض. هذه التقنية توفر راحة حقيقية للنساء اللواتي يعانين من أعراض مزعجة، وتحتفظ بالرحم بعكس الجراحة التقليدية التي قد تتطلب استئصاله.
كيف تتم قسطرة الرحم: خطوات الإجراء بالتفصيل
عملية تفاصيل قسطرة الرحم تتطلب دقة وخبرة عالية. إليك كيفية سير الإجراء:
الخطوة الأولى – التحضير: يتم إعطاء المريضة مخدر موضعي بدلاً من التخدير العام، مما يقلل المخاطر ويسرع التعافي.
الخطوة الثانية – الوصول الوعائي: يقوم الطبيب بإدخال قسطرة رفيعة عبر الشريان الفخذي، وهو أكبر شرايين الجسم.
الخطوة الثالثة – التوجيه بالأشعة: باستخدام تقنية الأشعة المتقدمة، يتم توجيه القسطرة بدقة نحو الشرايين المغذية للأورام.
الخطوة الرابعة – حقن المادة: يتم حقن جزيئات خاصة (Embolic agents) تقطع الدم عن الورم، مما يؤدي إلى ضموره.
المدة الإجمالية للإجراء عادة ما تكون 30-60 دقيقة، والمريضة تكون واعية طوال الوقت.
تفاصيل قسطرة الرحم: ما الذي يحدث بعد الإجراء
بعد انتهاء الإجراء مباشرة، تنتقل المريضة إلى غرفة الملاحظة حيث تبقى تحت الأشعة والمراقبة الطبية لضمان استقرارها.
يشعر معظم المريضات بـ تفاصيل قسطرة الرحم وتأثيراتها المبكرة في شكل:
تقلصات خفيفة في الرحم (طبيعية وتدل على استجابة الجسم)
شعور بدفء في البطن
ألم خفيف في موقع إدخال القسطرة
هذه الأعراض تختفي في غضون 24-48 ساعة.
قسطرة رفيعة: التطور التكنولوجي الذي غيّر قواعد اللعبة
استخدام قسطرة رفيعة للغاية يعتبر من أهم التطورات في هذا المجال. القسطرات الحديثة قطرها أصغر من سمك شعرة الرأس، مما يقلل من:
الألم أثناء الإدخال
خطر الإصابة بالجلطات
الكدمات والمضاعفات الموضعية
هذا التطور جعل الإجراء أكثر آماناً وراحة للمريضات، وأتاح للأطباء مستويات دقة أعلى.
علاج التليف الرحمي بالطرق التقليدية قد يتطلب إجراءات جراحية كبرى مثل استئصال الرحم أو إزالة الأورام جراحياً. لكن قسطرة الرحم للأورام الليفية تقدم بديلاً حقيقياً بدون جراحة:
المميزات
التفاصيل
عدم الحاجة للتخدير العام
تخدير موضعي فقط، أقل خطورة
وقت التعافي القصير
العودة للحياة الطبيعية في أيام
الحفاظ على الرحم
تبقى القدرة على الحمل محتملة
نسبة نجاح 95%
نتائج مثبتة وموثقة
الآثار السلبية لقسطرة الرحم: ما يجب أن تعرفيه
كأي إجراء طبي، هناك احتمالية لبعض الآثار الجانبية، لكن الأخبار السارة أنها نادرة جداً:
الآثار الجانبية الشائعة (والمؤقتة):
آلام خفيفة إلى متوسطة في البطن تستمر أياماً قليلة
إحساس بالتعب العام لمدة يومين
ارتفاع طفيف في درجة الحرارة (نادر)
المضاعفات النادرة جداً:
العدوى (أقل من 1%)
جلطات دموية (نادرة جداً مع التقنيات الحديثة)
حساسية من الصبغة الطبية المستخدمة
معظم هذه التأثيرات تختفي من تلقاء نفسها في غضون أسابيع قليلة، وطبيبك سيزودك بأدوية للتحكم في الألم والالتهاب.
الإجابة: لا، قسطرة الرحم ليست مؤلمة في الحقيقة. سيشعر لديك:
تخدير موضعي يزيل الألم من موقع الإدخال
ضغط خفيف أثناء إدخال القسطرة (وليس ألم)
بعض التقلصات الخفيفة أثناء الإجراء (تشبه تقلصات الدورة)
معظم المريضات يقلن أن الخوف كان أسوأ من الإجراء نفسه!
ما هو حجم الأورام الليفية التي تحتاج إلى عملية جراحية؟
الإجابة: في الواقع، حجم الورم ليس هو المعيار الأساسي. ما يهم هو:
الأعراض التي تسببها (نزيف، ألم، ضغط على المثانة)
موقع الورم في الرحم
عدد الأورام
تأثيره على الخصوبة
قسطرة الرحم للأورام الليفية يمكن أن تعالج أوراماً بأحجام مختلفة – صغيرة أو كبيرة. حتى الأورام الكبيرة التي قد تبدو بحاجة لجراحة يمكن علاجها بنسبة نجاح 95% باستخدام هذه التقنية.
الاستشارة مع طبيب متخصص هي الأساس لتحديد أفضل خيار لحالتك.
قسطرة الرحم للأورام الليفية لا تمنع الحمل بشكل مباشر. في الحقيقة:
الرحم يبقى سليماً وكاملاً (بعكس الجراحة)
الأنابيب تبقى مفتوحة وسليمة
المبايض لا تتأثر بالإجراء
النقطة المهمة: الأورام الليفية نفسها قد تؤثر على الخصوبة. بإزالة الأعراض والتخلص من الأورام، تزيد فرص الحمل الطبيعي.
معظم النساء اللواتي حملن بعد القسطرة يفعلن ذلك بدون مساعدة طبية إضافية.
ما هو أفضل علاج للالياف الرحمية؟
الإجابة: لا يوجد “علاج واحد الأفضل” – الأفضل هو ما يناسب حالتك الشخصية:
الخيارات المتاحة:
المتابعة المحافظة – إذا كانت الأعراض خفيفة جداً
الأدوية الهرمونية – تقلل الأعراض لكن لا تزيل الأورام
قسطرة الرحم للأورام الليفية – الحل المثالي لمعظم الحالات (نسبة نجاح 95%)
الجراحة التقليدية – للحالات النادرة جداً
قسطرة الرحم تعتبر الخيار الأفضل لأنها:
فعالة وآمنة
تحافظ على الرحم
توفر نتائج طويلة الأمد
تعافي سريع
التشاور مع متخصص مثل الدكتور سمير عبد الغفار يساعدك على اختيار الخيار الأمثل.
معلومات التواصل – اتخذي الخطوة الأولى
إذا كنتِ تعانين من أعراض الأورام الليفية وترغبين في اكتشاف كيف يمكن قسطرة الرحم للأورام الليفية أن تحسّن حياتك، فريق الدكتور سمير عبد الغفار هنا للمساعدة.
في لندن – المملكة المتحدة:
📞 رقم العيادة: 00442081442266 💬 WhatsApp: 00447377790644
في القاهرة – مصر:
📞 رقم حجز القاهرة: 00201000881336 💬 WhatsApp: 00201000881336
قسطرة الرحم للأورام الليفية ليست مجرد خيار طبي – إنها تحول حقيقي لحياة آلاف النساء. بفضل التقنيات الحديثة، تقنية الأشعة المتطورة، وقسطرة رفيعة آمنة، أصبح من الممكن علاج هذه الحالة بدون جراحة والحفاظ على الرحم والقدرة على الحمل.
مع نسبة نجاح 95% وتعافي سريع، لا حاجة للعيش مع الألم والنزيف الغزير. اتصلي بعيادة الدكتور سمير عبد الغفار اليوم وابدئي رحلتك نحو حياة خالية من الأعراض.
معلومات إضافية مهمة
✅ الاستشارة الأولية تتضمن فحصاً دقيقاً وشرحاً واضحاً لخيارات العلاج ✅ السرية التامة في جميع معاملاتك الطبية ✅ فريق طبي متخصص بخبرة عشرات السنوات ✅ معدلات نجاح عالية تدعمها دراسات عالمية
ملاحظة نهائية: المعلومات في هذا المقال مبنية على أحدث الدراسات الطبية والمبادئ العلمية. لكن هذا المقال لا يحل محل الاستشارة الطبية المباشرة. تحدثي دائماً مع طبيبك قبل اتخاذ أي قرار طبي.
Pain during your periods shouldn’t feel normal. Heavy bleeding that disrupts your daily life isn’t something you should accept. Yet thousands of women live with these symptoms, believing surgery is their only option. The truth? You can learn how to get rid of fibroids without surgery through proven alternatives that work.
Many women diagnosed with uterine fibroids fear they’ll need a hysterectomy. That’s understandable—but outdated. Modern medicine offers effective treatments that don’t require removing your uterus or going under the knife for major surgical procedures.
Can Fibroids Be Cured Permanently Without Surgery?
This question troubles many women facing a fibroid diagnosis. While fibroids are benign tumors that grow in the uterine muscle, the idea of “cure” needs clarification.
Fibroids don’t work like infections you can completely eliminate. However, non-surgical treatments can shrink them significantly, relieve your symptoms, and prevent new ones from causing problems. Think of it as managing the condition rather than chasing an absolute cure.
What actually works for permanent relief?
Uterine artery embolization blocks blood flow to fibroids, causing them to shrink
Focused ultrasound targets and destroys fibroid tissue
Hormonal treatments can manage growth in some cases
Natural approaches may help smaller, non-symptomatic fibroids
The key is finding what works for your specific situation—the size of your fibroids, their location, your symptoms, and your future plans matter.
How to Get Rid of Fibroids Without Surgery
Getting rid of fibroids without going through major surgery is more achievable than most people realize. The medical field has developed several minimally invasive procedures that offer real results.
This procedure has changed everything for women seeking alternatives to hysterectomy. During UAE, a specialist injects tiny particles into the arteries feeding your fibroids. Without blood supply, these tumors shrink naturally over the following months.
The benefits are remarkable:
Done through a small catheter—no large incisions
You keep your uterus intact
Recovery takes days, not weeks
Over 90% of women experience symptom relief
Pregnancy remains possible for many women
Focused Ultrasound Treatment
High-intensity focused ultrasound waves target fibroid tissue without cutting. It’s completely non-invasive, though it works best for certain types and locations of fibroids.
Medication Options
Gonadotropin-releasing hormone agonists can temporarily shrink fibroids by lowering hormone levels. While not permanent, they offer relief and can help you avoid surgical intervention while planning your next steps.
How to Shrink Fibroids Naturally Without Surgery
Natural approaches won’t replace medical treatment for symptomatic fibroids, but they can help manage smaller ones and support your overall health.
Lifestyle Changes That Matter
Your daily habits affect fibroid growth more than you might think. Women who maintain a healthy weight often experience fewer symptoms. Regular exercise helps balance hormones and reduce inflammation.
Stress Management
Chronic stress elevates cortisol, which can influence fibroid development. Finding ways to relax—whether through meditation, yoga, or simply taking breaks—supports your body’s natural balance.
Natural Supplements
Some people find relief using:
Green tea extract
Vitamin D supplementation
Curcumin (found in turmeric)
Fish oil for anti-inflammatory benefits
Always discuss supplements with your doctor before starting, especially if you’re taking other medicine or planning pregnancy.
Fibroid Removal Without Surgery
When people talk about “fibroid removal,” they usually imagine surgical procedures. But several minimally invasive options exist that don’t require traditional surgery.
This procedure, offered by interventional radiology specialists like Dr. Samir Abdel Ghaffar, removes the fibroid’s blood supply rather than cutting it out. The result? Fibroids shrink and symptoms disappear without the risks of major surgery.
The procedure takes about an hour. You’ll have a small incision in your groin or wrist where the catheter enters. Most women go home the same day.
What Makes UFE Different?
Unlike surgical removal, UFE:
Treats all fibroids at once, regardless of number
Preserves the uterus completely
Requires no general anesthesia in most cases
Offers faster recovery than traditional options
Reduces risk of fibroid recurrence
Best Treatment for Fibroids
The “best” treatment depends entirely on your situation. What works beautifully for one woman might not suit another.
Factors Your Doctor Should Consider:
Size and location of your fibroids
Severity of symptoms you’re experiencing
Your age and whether you want future pregnancy
Overall health conditions
Personal preferences about treatment approach
Comparing Your Options
For symptomatic fibroids causing heavy bleeding and pain, uterine artery embolization often emerges as the most effective treatment. It balances efficacy with minimal invasion, offering relief without the recovery time of abdominal hysterectomy.
Hysterectomy removes the uterus entirely—a definitive solution, but one that ends fertility and requires major surgery. Many women who choose hysterectomy later discover they could have preserved their uterus through alternatives.
Myomectomy removes individual fibroids while keeping the uterus. It requires surgical incisions and fibroids can return, but some women prefer this approach.
Fibroid Removal Without Surgery Cost
Treatment costs vary significantly based on location, procedure type, and insurance coverage.
Understanding the Financial Picture
Non-surgical fibroid removal options like UFE typically cost less than traditional surgery when you factor in:
Shorter hospital stays (often same-day discharge)
Faster return to work
Lower complication rates
No need for extended recovery care
Many insurance plans cover uterine fibroid embolization, recognizing it as an effective alternative to surgical procedures. Check with your provider about specific coverage.
For consultations with Dr. Samir Abdel Ghaffar regarding treatment options and costs:
In London, UK:
Clinic: 00442081442266
WhatsApp: 00447377790644
In Cairo, Egypt:
Booking: +201000881336
WhatsApp: +201000881336
How to Remove Fibroid Naturally at Home 🌿
Complete fibroid removal at home isn’t realistic—these are physical tumors growing in your uterine muscle. However, you can manage symptoms and potentially slow growth through home-based approaches.
Daily Habits That Help:
Start your day with anti-inflammatory foods. Add ginger to your morning tea. Choose whole grains over processed options. These small changes support hormonal balance.
Heat Therapy
A heating pad on your lower abdomen can relieve cramps and pelvic discomfort during periods. While it doesn’t remove fibroids, it manages the pain they cause.
Herbal Support
Some women find relief using:
Chasteberry (may help balance hormones)
Milk thistle (supports liver function and hormone metabolism)
Dandelion root (aids detoxification)
Remember: natural doesn’t mean risk-free. Discuss any herbal remedies with your healthcare provider.
Treatment of Fibroid Without Surgery
Modern treatment of fibroid without surgery centers on minimally invasive procedures that target the root problem.
Uterine Artery Embolization: The Gold Standard 💫
Dr. Samir Abdel Ghaffar specializes in this procedure, offering women a proven alternative to hysterectomy. As a consultant in interventional radiology, he performs UAE using advanced catheterization techniques.
The Procedure Process:
You’ll receive local anesthesia and mild sedation. A tiny tube goes into an artery in your wrist or groin. Using X-ray guidance, the doctor navigates to the arteries feeding your fibroids and injects small particles that block blood flow.
Without their blood supply, fibroids begin shrinking within weeks. Most women notice symptom improvement within the first month, with maximum results appearing over three to six months.
Recovery Reality:
Most women rest for a few days
Return to normal activities within a week
Avoid heavy lifting for two weeks
Full recovery typically takes one month
Compare this to surgical options requiring six to eight weeks of recovery.
7 Foods for Shrinking Fibroids
While food alone won’t eliminate fibroids, certain dietary choices support your body in managing them.
1. Leafy Greens
Spinach, kale, and collard greens provide iron (important if you have heavy bleeding) and support liver function for hormone balance.
2. Fatty Fish
Salmon, mackerel, and sardines offer omega-3 fatty acids that reduce inflammation and may slow fibroid growth.
3. Whole Grains
Brown rice, quinoa, and oats provide fiber that helps your body eliminate excess hormones. They also stabilize blood sugar, which affects hormone production.
4. Legumes
Beans and lentils offer plant-based protein and fiber. They’re filling, nutritious, and support hormone balance.
5. Cruciferous Vegetables
Broccoli, cauliflower, and Brussels sprouts contain compounds that help your body metabolize estrogen more effectively.
6. Berries 🫐
Blueberries, strawberries, and raspberries provide antioxidants that fight inflammation and support overall health.
7. Green Tea
Rich in EGCG, a compound that may inhibit fibroid growth. Aim for two to three cups daily.
Foods to Limit:
Red meat (linked to increased fibroid risk)
Processed foods high in added sugars
Alcohol (affects hormone metabolism)
High-fat dairy products
Understanding Your Treatment Options
Choosing how to proceed with fibroid treatment affects your health, fertility, and quality of life. Understanding all available options empowers better decisions.
Minimally Invasive Procedures
These treatments offer middle ground between doing nothing and major surgery. They include:
Uterine Fibroid Embolization (UFE): Blocks blood supply to fibroids through catheterization. Highly effective for most women regardless of fibroid size or number.
MRI-Guided Focused Ultrasound: Uses ultrasound waves to destroy fibroid tissue. Works best for fibroids in certain locations within the uterus.
Radiofrequency Ablation: Destroys fibroid tissue using heat energy. Requires small incisions but isn’t technically major surgery.
When Surgery Becomes Necessary
Some situations genuinely require surgical intervention:
Fibroids causing severe anemia despite treatment
Rapid growth requiring tissue diagnosis
Fibroids affecting other organs
Failure of minimally invasive treatments
Even then, myomectomy (removing just the fibroids) often works better than hysterectomy for women wanting to preserve fertility.
Frequently Asked Questions
How can I naturally break down my fibroids?
Your body can’t completely break down fibroids naturally, but lifestyle changes help manage them. Focus on anti-inflammatory foods, maintain healthy weight, exercise regularly, and manage stress. These approaches support hormonal balance and may slow growth. For actual shrinkage, you’ll need medical treatment like UAE.
What pills shrink fibroids?
Gonadotropin-releasing hormone agonists temporarily shrink fibroids by reducing estrogen. Birth control pills don’t shrink fibroids but can manage heavy bleeding. Tranexamic acid reduces bleeding during periods. Anti-prostaglandin medications relieve pain and cramps. Your doctor will recommend the best medicine based on your symptoms.
What makes fibroids stop growing?
Fibroids grow in response to hormones, particularly estrogen and progesterone. They typically stop growing during menopause when hormone levels drop. Treatments like GnRH agonists create temporary menopause-like conditions. UAE cuts off blood supply, causing fibroids to shrink and stop growing. Maintaining healthy hormone balance through lifestyle may slow growth.
What to drink to flush out fibroids?
No drink can “flush out” fibroids—they’re solid tumors in your uterine muscle. However, green tea contains compounds that may inhibit fibroid growth. Water helps your body function optimally. Avoid alcohol, which can affect hormone metabolism. Focus on medical treatments that actually shrink fibroids rather than seeking miracle drinks.
What size fibroids need surgery?
Size alone doesn’t determine whether you need surgery. A large fibroid causing no symptoms might not require treatment, while a small one pressing on your bladder could need intervention. Generally, fibroids over 10 cm often require treatment. However, your symptoms, fibroid location, and future pregnancy plans matter more than size alone. Many women with large fibroids benefit from UAE rather than surgery.
Which food can remove fibroids?
No food removes fibroids. However, certain foods support fibroid management: leafy greens provide nutrients and support hormone balance; fatty fish offers anti-inflammatory omega-3s; cruciferous vegetables help metabolize estrogen; legumes provide fiber for hormone elimination; berries fight inflammation. These foods complement medical treatment but don’t replace it.
What happens if I don’t remove my fibroids?
Small, non-symptomatic fibroids often require no treatment. Many women live normally with fibroids. However, symptomatic fibroids can cause heavy bleeding leading to anemia, severe pelvic pain affecting daily life, frequent urination from bladder pressure, constipation from pressure on intestines, and potential pregnancy complications. Treatment prevents these issues and improves quality of life.
What are the main causes of fibroids?
Doctors don’t know exactly what causes fibroids, but several factors contribute: hormones (estrogen and progesterone) promote fibroid growth, genetic factors play a role, early menstruation increases risk, family history matters significantly, obesity and diet affect risk, and vitamin D deficiency shows correlation. Most women develop some fibroids during reproductive years.
Which vitamin shrinks fibroids?
Vitamin D shows promise in fibroid management. Studies suggest women with adequate vitamin D levels have lower fibroid risk. Supplementation may slow growth but won’t dramatically shrink existing fibroids. Always consult your doctor about appropriate dosing. Other nutrients like B vitamins support hormone metabolism. However, vitamins work best as part of comprehensive treatment, not standalone solutions.
Taking Control of Your Fibroid Treatment
Living with symptomatic fibroids affects every aspect of your life—from missing work due to heavy periods to avoiding activities because of pain. You don’t have to accept this as normal, and you definitely don’t need to lose your uterus to find relief.
Uterine artery embolization offers a middle path. It’s effective enough to eliminate symptoms yet gentle enough to preserve your fertility and avoid major surgery. Women who choose UAE typically experience dramatic improvement in their quality of life without the risks and recovery time of traditional surgery.
Dr. Samir Abdel Ghaffar has helped countless women discover this alternative. As a consultant in interventional radiology with extensive experience in catheterization techniques, he provides expert care for fibroid treatment without surgery.
Your next steps:
Schedule a consultation to discuss your specific situation
Learn about UFE and whether it’s right for you
Understand recovery expectations and timeline
Make an informed decision about your health
Contact Dr. Samir Abdel Ghaffar:
London, UK:
Clinic: 00442081442266
WhatsApp: 00447377790644
Cairo, Egypt:
Booking: +201000881336
WhatsApp: +201000881336
Don’t let fibroids control your life. Effective treatment exists that respects your body, preserves your options, and gets you back to living fully. The alternative to hysterectomy you’ve been searching for is here—and it works.
Every month, millions of women experience unexplained pelvic discomfort, wondering what’s happening inside their bodies. The heavy bleeding disrupts your daily routine, the pressure makes simple activities uncomfortable, and the uncertainty leaves you searching for answers. If you’ve recently discovered growths in your uterus, you’re probably feeling overwhelmed by medical terminology and concerned about what comes next.
Understanding the different types of fibroids in uterus can be your first step toward reclaiming control of your health. These benign muscle growths affect up to 70% of women by age 50, yet many don’t realize they have options beyond major surgery. This guide breaks down everything you need to know about uterine fibroids, their classification, and modern treatment approaches that preserve your reproductive organs.
What Are the Different Types of Fibroids in Uterus?
Uterine fibroids, also called leiomyomas, are noncancerous tumors that develop from the smooth muscle tissue of the uterus. While the term “tumor” might sound alarming, these growths are benign and rarely become cancerous. The anatomical classification of uterine fibroids is based primarily on their location within or around the uterus.
The main types of fibroids include:
Intramural fibroids
These grow within the muscular wall of the uterus itself, making them the most common type. They can cause the uterus to appear enlarged and may lead to heavy menstrual bleeding.
Located on the outer wall of the uterus, these masses can grow large enough to make your uterus appear bigger on one side. They typically cause pressure symptoms rather than bleeding issues.
Submucosal fibroids
These develop just beneath the lining of the uterine cavity and bulge into the space where a baby would grow. Even small submucosal growths can cause significant bleeding and fertility challenges.
Pedunculated fibroids
Whether subserosal or submucosal, some fibroids grow on small stalks called peduncles, giving them a mushroom-like appearance.
The FIGO classification system provides a more detailed approach, numbering fibroids from 0-8 based on their specific location and how much they extend into different layers of the uterus.
Types of Fibroids and Their Location: Where Do They Develop?
Understanding where fibroids grow helps explain why different women experience vastly different symptoms. Your uterus has several layers – the inner lining (endometrium), the thick muscular wall (myometrium), and the outer covering (serosa). Fibroids can originate from any of these areas.
Within the muscular wall – Intramural fibroids make up about 70% of all cases. Because they grow inside the uterus wall, they can distort both the outer shape and inner cavity as they expand.
Beneath the outer surface – Subserosal types extend outward from the uterus toward your pelvic cavity. These can press against your bladder, causing frequent urination, or push on your rectum, leading to constipation.
Under the cavity lining – Submucosal fibroids are less common but often cause the most troublesome bleeding. They can project into your uterine cavity, sometimes growing large enough to fill the entire space.
Near the cervix – Cervical fibroids develop in the wall of the cervix rather than the main body of the uterus. They’re relatively rare but can complicate childbirth.
The location matters tremendously when determining treatment strategies. A fibroid pressing on your bladder creates different challenges than one causing heavy periods, even if they’re the same size.
Which Type of Fibroid Is Dangerous? Understanding Risk Levels
Most women worry about cancer when they hear they have tumors. Here’s the reassuring truth: fibroids are cancerous in fewer than 1 in 1,000 cases. The condition called leiomyosarcoma is a separate, rare cancer that can develop in the uterus but isn’t actually a fibroid that “turned bad.”
However, certain characteristics deserve attention:
Rapidly growing masses – While most fibroids grow slowly, those that enlarge quickly, especially after menopause, warrant closer examination to rule out other conditions.
Submucosal types causing severe bleeding – These can lead to anemia serious enough to require blood transfusions if left untreated. The constant blood loss impacts your energy, concentration, and overall quality of life.
Large subserosal fibroids – When these reach grapefruit size or larger, they can press on organs, potentially affecting kidney function if they block the ureters (tubes connecting kidneys to bladder).
Pedunculated fibroids – Those on stalks occasionally twist, cutting off their blood supply. This causes sudden, severe pain requiring emergency treatment.
The “danger” usually relates more to quality of life than actual cancer risk. Chronic pain, debilitating bleeding, or organ pressure significantly impact your daily activities, relationships, and mental health – concerns just as valid as any medical emergency.
Is Intramural Fibroid Dangerous? What You Should Know
Intramural fibroids represent the most common type, growing within the uterus wall itself. Their danger level depends entirely on their size, number, and impact on your body rather than their classification.
Small intramural growths often cause no symptoms whatsoever. Many women discover them incidentally during ultrasounds for other reasons. However, as these fibroids grow, they can:
Distort the uterine cavity, potentially affecting fertility or pregnancy
Cause the uterus to enlarge, creating a feeling of fullness or pressure
Lead to heavier, longer menstrual periods as they interfere with normal uterine contractions
Press on surrounding structures as they expand outward
The real concern with intramural fibroids isn’t danger in a life-threatening sense, but rather their potential to grow multiple inches in diameter. A 10-centimeter intramural fibroid can make your uterus the size of a four-month pregnancy, causing visible abdominal swelling and significant discomfort.
Your body’s estrogen levels influence how these growths behave. During reproductive years when estrogen is high, intramural fibroids may grow steadily. After menopause, when estrogen drops, they typically shrink on their own – which is why monitoring is sometimes a reasonable approach for women nearing perimenopause.
Treatment of Fibroid: Modern Approaches Beyond Hysterectomy 💡
For decades, women faced limited choices: live with symptoms or remove the entire uterus. Today’s treatment landscape offers far more options, especially for those wanting to preserve their reproductive organs.
Watchful waiting works well when fibroids cause minimal symptoms. Regular monitoring ensures any changes are caught early.
Medications can help manage symptoms temporarily. Hormonal treatments may reduce bleeding, while pain relievers address discomfort. However, these don’t eliminate the growths themselves.
Myomectomy surgically removes individual fibroids while leaving the uterus intact. This option appeals to women desiring future pregnancy, though fibroids can regrow over time.
Uterine Artery Embolization (UAE) represents a breakthrough in fibroid management. This minimally invasive procedure blocks blood flow to fibroids, causing them to shrink. Dr. Samir Abdel Ghaffar specializes in this technique, which requires no major incision, preserves the uterus, and allows most women to return home the same day.
During UAE, tiny particles are injected through a catheter into the arteries feeding the fibroids. Without their blood supply, the growths shrink by an average of 50% over several months. Symptoms improve in about 90% of women, with most experiencing dramatic relief from bleeding and pressure within weeks.
Hysterectomy – complete removal of the uterus – remains an option but should be considered carefully. While it permanently resolves fibroid symptoms, it’s major surgery with significant recovery time and ends any possibility of pregnancy.
The best treatment depends on your specific situation: fibroid type and location, symptom severity, desire for future children, and personal preferences about surgery and recovery time.
Subserosal Fibroid: Symptoms and Management
Subserosal fibroids grow on the outer uterine wall, extending into the pelvic cavity. Because they develop away from the uterine lining, they rarely cause the heavy menstrual bleeding associated with other types.
Instead, women with subserosal growths typically experience:
Pressure symptoms – As these fibroids expand outward, they press on nearby organs. You might feel like you constantly need to urinate, even when your bladder isn’t full. Constipation can develop if fibroids press against your rectum.
Pelvic discomfort – Large subserosal fibroids create a sensation of fullness or heaviness in your lower abdomen. Some women describe it as feeling perpetually bloated.
Back pain – When located on the posterior (back) wall of the uterus, these masses can press on nerves, causing lower back pain that worsens with certain positions.
Visible swelling – Subserosal fibroids can grow quite large before causing symptoms. Some reach the size of a melon, creating noticeable abdominal enlargement that’s often mistaken for weight gain.
Pain during sex – Depending on their position, these fibroids can make intercourse uncomfortable, particularly with deep penetration.
Managing subserosal fibroids depends on symptom severity. Small, asymptomatic ones may simply be monitored. When they cause significant pressure or pain, minimally invasive treatments like uterine artery embolization effectively shrink them without requiring major surgery. Unlike fibroids that distort the uterine cavity, subserosal types rarely affect fertility directly, though extremely large ones might complicate pregnancy.
Intramural Fibroid Ultrasound: How Diagnosis Works
Ultrasound remains the primary tool for detecting and evaluating intramural fibroids. This painless imaging technique uses sound waves to create pictures of your uterus, revealing the number, size, and location of any growths present.
Transabdominal ultrasound involves moving a device called a transducer across your lower abdomen. You’ll need a full bladder for this exam, as it helps create clearer images. This approach works well for viewing larger fibroids and getting an overall picture of your uterus.
Transvaginal ultrasound provides more detailed images, especially of smaller fibroids and those near the uterine lining. A slender probe is gently inserted into the vagina, allowing the ultrasound to get much closer to the uterus. While some women feel anxious about this exam, most find it causes minimal discomfort.
On ultrasound images, intramural fibroids typically appear as round or oval masses with defined edges within the uterine wall. The muscular wall itself may look thickened or irregular if multiple fibroids are present.
Sometimes additional imaging is needed:
MRI scans provide the most detailed view, showing exact fibroid locations and helping plan treatment approaches. They’re particularly useful before procedures like UAE or myomectomy.
Sonohysterography involves injecting sterile fluid into the uterus during ultrasound, creating better visualization of the uterine cavity and any submucosal components.
Hysteroscopy uses a thin camera inserted through the cervix to directly view the inside of the uterus, perfect for examining submucosal fibroids.
The diagnosis process typically begins with your description of symptoms, followed by a pelvic exam where your doctor feels for an enlarged or irregularly shaped uterus. Ultrasound then confirms the presence of fibroids and provides essential information about their characteristics.
Intramural Fibroid Treatment: Tailored Solutions
Because intramural fibroids are so common and vary widely in size and impact, treatment must be individualized. What works perfectly for one woman might not suit another, even with similar fibroid characteristics.
For small, asymptomatic intramural fibroids, observation is often the wisest course. Regular check-ups ensure they’re not growing rapidly or beginning to cause problems. This conservative approach avoids unnecessary interventions.
Hormonal medications can help control symptoms temporarily. Birth control pills, hormonal IUDs, or GnRH agonists may reduce heavy bleeding and shrink fibroids somewhat. However, most resume growing once medication stops, making this a short-term solution.
Uterine artery embolization excels at treating intramural fibroids of various sizes. The procedure works by blocking blood flow to the fibroids while preserving circulation to healthy uterine tissue. Over subsequent weeks and months, the oxygen-starved fibroids shrink and symptoms improve dramatically. 🌟
Dr. Samir Abdel Ghaffar has helped countless women avoid hysterectomy through this minimally invasive approach. The procedure requires only local anesthesia and a tiny puncture in your groin or wrist – no large incisions. Most women go home the same day and return to normal activities within a week.
Myomectomy surgically removes individual fibroids while preserving the uterus. This option appeals particularly to women planning future pregnancies. However, surgery carries more risks than UAE, requires longer recovery, and doesn’t prevent new fibroids from developing.
Hysterectomy or supracervical hysterectomy (removing the uterus while leaving the cervix) provides permanent relief but ends fertility and requires major surgery with significant recovery time.
The choice between these approaches depends on multiple factors: how much fibroids affect your daily life, whether you plan to have children, your overall health, and your preferences regarding surgery and recovery.
Prevention of Uterine Fibroid: Can You Reduce Your Risk?
While you can’t completely prevent fibroids, understanding risk factors helps you make informed choices that might reduce your likelihood of developing them or slow their growth.
Factors beyond your control include:
Family history – if your mother or sister had fibroids, your risk increases
Age – fibroids are most common during reproductive years
Ethnicity – they develop more frequently and at younger ages in women of African descent
Modifiable factors you can address:
Maintain a healthy weight – Obesity increases fibroid risk because fat tissue produces estrogen. Even modest weight loss can help, as excess estrogen promotes fibroid growth.
Eat more vegetables and fruits – Diets rich in green vegetables appear protective. Some research suggests vitamin D supplementation might reduce risk, though more studies are needed.
Limit red meat and alcohol – Both have been associated with higher fibroid rates in some studies, while fish consumption shows potential protective effects.
Exercise regularly – Physical activity helps maintain healthy weight and may reduce estrogen levels, potentially lowering fibroid risk.
Consider vitamin D – Some evidence suggests adequate vitamin D levels might offer protection, though this research is still developing.
Manage stress – While not directly proven to cause fibroids, chronic stress affects hormone balance throughout your body.
Understand birth control effects – Long-term use of birth control pills might slightly reduce risk, though this area needs more research.
It’s important to remember that even with perfect lifestyle choices, some women still develop fibroids due to genetic factors and hormonal influences beyond anyone’s control. If fibroids do develop, focus shifts from prevention to appropriate management.
Living with Fibroids: Impact on Daily Life and Relationships
Beyond medical terminology and treatment options, fibroids affect real women living real lives. The physical symptoms often extend into emotional, social, and relationship challenges that deserve acknowledgment.
Heavy bleeding can make you afraid to leave home during your period, worried about accidents at work or social events. The constant need to change protection, combined with severe cramping, disrupts sleep and concentration. Many women develop anemia from chronic blood loss, leading to exhaustion that affects every aspect of life.
Pelvic pressure and pain can interfere with exercise, making it difficult to maintain fitness or enjoy physical activities you once loved. Some women feel self-conscious about abdominal swelling from large fibroids, affecting their body image and clothing choices.
Intimate relationships face strain when fibroids cause pain during sex. The combination of physical discomfort, heavy bleeding, and fatigue can reduce desire and create distance between partners. Open communication becomes essential, yet many women feel embarrassed discussing these issues.
Fertility concerns weigh heavily on women hoping to have children. While many with fibroids conceive and carry pregnancies successfully, uncertainty about whether these growths will interfere creates anxiety and stress.
The good news is that effective treatment dramatically improves quality of life. Women who undergo procedures like uterine artery embolization often report feeling like they’ve reclaimed their lives – no more planning activities around bleeding schedules, no more chronic exhaustion, and renewed confidence in their bodies.
Frequently Asked Questions About Fibroids
What are the 4 types of fibroids?
The four main types are intramural (within the uterine wall), subserosal (on the outer surface), submucosal (beneath the cavity lining), and pedunculated (attached by a stalk). These classifications are based on where the fibroid grows in relation to the uterine structure.
What type of fibroids need to be removed?
Fibroids requiring removal are those causing significant symptoms like severe bleeding, anemia, pain, or organ pressure. Submucosal fibroids often need treatment even when small because they interfere with the uterine cavity. Large fibroids of any type that affect quality of life also warrant removal or other intervention.
What is type 7 fibroid?
In the FIGO classification system, type 7 fibroids are subserosal growths attached to the outer uterine wall by more than 50% of their diameter. This detailed classification helps doctors plan appropriate treatment approaches.
Can fibroids cause leg swelling?
Yes, very large fibroids can press on blood vessels or lymph nodes in the pelvis, potentially causing swelling in the legs. However, this is uncommon and usually only occurs with quite large masses. If you experience leg swelling, consult your doctor to rule out other causes.
What are the worst fibroids to have?
Submucosal fibroids are often considered the most problematic because even small ones cause heavy bleeding and can significantly impact fertility. Large intramural fibroids that distort the uterine cavity also create substantial challenges. However, “worst” really depends on individual circumstances and symptoms.
Which type of fibroids are cancerous?
Fibroids themselves are benign, not cancerous. Leiomyosarcoma is a rare cancer that can develop in the uterus but is a different condition entirely, not a fibroid that became malignant. True cancerous transformation of a benign fibroid is extremely rare.
At what stage should fibroids be removed?
Removal or treatment should be considered when fibroids cause symptoms that significantly affect your quality of life, lead to anemia from heavy bleeding, interfere with fertility or pregnancy, or grow rapidly. Asymptomatic fibroids can often be monitored without intervention.
What are the main causes of fibroids?
The exact cause remains unknown, but genetic factors, hormones (especially estrogen and progesterone), and growth factors all play roles. Family history, age, obesity, and ethnicity influence risk. They’re not caused by anything you did wrong or could have prevented.
What happens if fibroids are not removed?
Many women live with small, asymptomatic fibroids without problems. However, untreated symptomatic fibroids can lead to chronic anemia, ongoing pain, fertility challenges, or organ complications from pressure. Most fibroids shrink naturally after menopause when hormone levels drop.
Which type of fibroid is most difficult to remove?
Large intramural fibroids deeply embedded in the uterine wall present the greatest surgical challenge. Multiple fibroids scattered throughout the uterus can also complicate surgical removal. This is one reason many doctors and patients prefer uterine artery embolization, which treats all fibroids simultaneously regardless of size or location.
What type of fibroids cause the most pain?
Pedunculated fibroids can cause sudden severe pain if they twist. Submucosal fibroids sometimes try to expel themselves from the uterus, causing intense cramping. Large fibroids pressing on organs or nerves create chronic pelvic pain. Pain severity varies greatly between individuals.
Why Choose Uterine Artery Embolization with Dr. Samir Abdel Ghaffar
When facing fibroid treatment decisions, you deserve options that preserve your health while effectively addressing symptoms. Uterine artery embolization offers a middle path between watchful waiting and major surgery.
Dr. Samir Abdel Ghaffar brings extensive expertise in interventional radiology to fibroid treatment. His specialized training in catheter-based procedures allows him to access and treat fibroids through blood vessels, avoiding large incisions entirely.
The advantages of choosing UAE include:
Uterus preservation for women wanting future pregnancy or simply preferring to keep their organs
Treating all fibroids simultaneously, regardless of number or location
Minimal recovery time compared to surgery – most patients return to work within a week
Low complication rates with experienced practitioners
No general anesthesia required
Same-day or overnight procedures without lengthy hospital stays
Patients consistently report dramatic symptom improvement within weeks, with full results evident over several months as fibroids continue shrinking.
If you’re struggling with fibroid symptoms and want to explore alternatives to hysterectomy, contact Dr. Samir Abdel Ghaffar to discuss whether uterine artery embolization suits your situation. 💪
In London, UK:
Clinic: 00442081442266
WhatsApp: 00447377790644
In Egypt:
Cairo Booking: +201000881336
WhatsApp: +201000881336
Your journey toward symptom relief and improved quality of life begins with understanding your options and choosing the approach that aligns with your goals and values. Don’t let fibroids control your life when effective, minimally invasive solutions exist.
Waking up to find your sheets stained, changing pads every hour, and passing blood clots the size of golf balls isn’t just inconvenient—it’s terrifying. You’re exhausted, anemic, and worried about what’s happening inside your body.
Every month, the bleeding gets worse. You cancel plans, miss work, and live in fear of embarrassing accidents. The clots are alarming, and you’re wondering if this is normal or something more serious.
Understanding the reasons for why do fibroids cause heavy bleeding and clots is your first step toward relief. The good news? You have treatment options that don’t involve major surgery.
Why Do Fibroids Cause Heavy Bleeding and Clots?
Fibroids trigger excessive menstrual bleeding through several mechanisms. These noncancerous growths in your uterus disrupt the normal menstrual cycle in ways that directly affect blood flow.
First, fibroids increase the surface area of the uterine lining. Think of your uterus as a room—fibroids push against the walls, stretching them and creating more space. When menstruation occurs, there’s simply more lining to shed, which means more bleeding.
Second, fibroids interfere with the uterus’s natural ability to contract. During your period, the uterus normally squeezes to close off blood vessels and control bleeding. Fibroids block these contractions, leaving vessels open and bleeding unchecked.
The location of the fibroids plays a crucial role too. Submucosal fibroids—those growing into the uterine cavity—are the greatest predictor of heavy bleeding. They sit right where menstrual blood collects, directly disrupting the endometrial lining and preventing proper healing.
Blood clots form when bleeding is so heavy that your body’s anticoagulants can’t keep up. The blood pools inside the uterus before being expelled, giving it time to clot. These clots can range from small specks to masses larger than a quarter.
Why Do Fibroids Cause Bleeding Between Periods?
Spotting or bleeding between periods is a common fibroid symptom that catches many women off guard. This happens because fibroids can erode the blood vessels in your uterine wall.
Submucosal fibroids, in particular, can develop a rich blood supply that becomes fragile and prone to spontaneous bleeding. You might notice pink or brown discharge, light spotting, or even heavier bleeding that seems to come out of nowhere.
The pressure from larger fibroids can also cause the endometrial lining to break down irregularly, leading to unpredictable bleeding patterns. Some patients report bleeding after exercise, sex, or even without any apparent trigger.
If you’re experiencing bleeding between periods, track the pattern. Note when it happens, how heavy it is, and any associated symptoms like pain or cramping. This information helps your doctor determine the best treatment approach.
How to Stop Heavy Bleeding from Fibroids
Managing heavy menstrual bleeding from fibroids involves both immediate relief strategies and long-term solutions.
Immediate measures:
Tranexamic acid tablets can reduce bleeding by up to 50% during your period
Hormonal birth control may lighten periods, though results vary
Iron supplements combat anemia from chronic blood loss
NSAIDs like ibuprofen can decrease flow and relieve cramping
Long-term treatment options:
Uterine artery embolization (UAE) offers a minimally invasive alternative to surgery. This procedure blocks blood flow to fibroids, causing them to shrink. Most women experience significant reduction in bleeding within three months.
Unlike hysterectomy, UAE preserves your uterus and requires only a tiny puncture in your wrist or groin. You’ll return home the same day and resume normal activities within a week.
Dr. Samir Abdel Ghaffar specializes in this advanced technique, helping women avoid major surgery while effectively treating their symptoms.
Why Do Fibroids Cause Bleeding After Menopause?
Finding blood after menopause is alarming because periods should have stopped. While fibroids typically shrink after menopause due to dropping estrogen levels, they can still cause bleeding in certain situations.
Postmenopausal bleeding from fibroids usually occurs when:
You’re taking hormone replacement therapy that stimulates fibroid growth
A submucosal fibroid begins to degenerate or break down
The fibroid has an unusually rich blood supply that remains active
Any postmenopausal bleeding requires immediate medical evaluation. While fibroids are a common cause, your doctor needs to rule out other conditions. Don’t wait or assume it’s nothing serious.
Fibroids and Blood Clots in Period
The connection between uterine fibroids and blood clots during menstruation is direct and significant. When you’re passing clots regularly, it’s your body’s response to overwhelming blood volume.
Normal menstrual blood contains anticoagulants that prevent clotting. But when bleeding exceeds what these anticoagulants can handle, blood pools and clots form. The size and frequency of clots often correlate with fibroid size and location.
Women with fibroids in the uterine cavity typically pass more clots than those with fibroids in the uterine wall. This happens because blood collects in the cavity before being expelled, giving it more time to clot.
Passing occasional small clots is normal. However, if you’re regularly seeing clots larger than a quarter, soaking through pads in less than two hours, or feeling dizzy and weak, you need medical attention.
Are Fibroid Clots Dangerous?
The clots themselves aren’t dangerous, but what they represent can be. Large, frequent clots signal excessive blood loss that can lead to serious complications.
Anemia is the most common danger. Chronic heavy bleeding depletes your iron stores, leaving you exhausted, weak, and short of breath. Severe anemia can affect your heart and other organs.
Warning signs that require immediate attention:
Soaking through a pad or tampon every hour for several hours
Passing clots larger than a golf ball
Feeling faint, dizzy, or experiencing heart palpitations
Severe abdominal pain accompanying the bleeding
Bleeding that doesn’t slow down after two days of your heaviest flow
These symptoms suggest your bleeding has crossed from manageable to dangerous. Don’t tough it out or wait for your next scheduled appointment.
What Causes Fibroids?
The exact cause of fibroids remains somewhat mysterious, but researchers have identified several contributing factors:
Hormonal influence: Estrogen and progesterone stimulate fibroid growth. These growths contain more hormone receptors than normal uterine tissue, making them especially responsive to hormonal fluctuations.
Genetic factors: If your mother or sister had fibroids, your risk increases significantly. Certain genetic mutations also predispose women to fibroid development.
Growth factors: Substances like insulin-like growth factor may play a role in fibroid formation and growth.
Additional risk factors include:
Being of African descent (fibroids are 2-3 times more common)
Starting your period early
Never having been pregnant
Obesity
Vitamin D deficiency
Diet high in red meat and low in fruits and vegetables
Understanding these risk factors doesn’t prevent fibroids, but it helps you monitor for symptoms and seek early treatment.
Can Fibroids Cause Blood Clots in Legs?
This is a crucial distinction: fibroids cause blood clots during menstruation, but they don’t typically cause dangerous blood clots in your legs (deep vein thrombosis or DVT).
However, very large fibroids—those bigger than a grapefruit—can occasionally press on pelvic blood vessels, potentially affecting circulation. This is rare and usually requires truly massive fibroids.
The real concern about leg clots comes from surgical treatment of fibroids. Any surgery, including hysterectomy or myomectomy, carries a small risk of DVT. This is one reason why minimally invasive treatments like uterine artery embolization are attractive—they carry significantly lower risks.
If you experience leg swelling, pain, warmth, or redness, seek immediate medical care. These symptoms could indicate a blood clot and require urgent evaluation.
Signs of Fibroids Breaking Down
Fibroid degeneration happens when a fibroid outgrows its blood supply and begins to break down. This process causes distinct symptoms:
Acute pain: Sharp, severe abdominal pain that comes on suddenly is the hallmark sign. The pain may be constant or come in waves.
Fever: Low-grade fever sometimes accompanies degeneration as your body responds to the dying tissue.
Increased bleeding: Some women experience heavier bleeding or spotting as the fibroid breaks down.
Tenderness: Your abdomen may feel tender to touch, especially over the fibroid location.
Most degenerating fibroids can be managed with pain medication and rest. The process typically resolves within a few weeks. However, severe pain or fever above 101°F warrants medical evaluation to rule out infection or other complications.
Uterine artery embolization intentionally causes controlled fibroid degeneration by cutting off blood supply. The difference is that this happens in a planned, monitored way that minimizes discomfort and maximizes benefit.
Understanding Heavy Menstrual Bleeding and Treatment Options
Heavy menstrual bleeding (menorrhagia) affects roughly one-third of women with fibroids. The impact goes far beyond inconvenience—it affects your quality of life, relationships, career, and overall health.
Menorrhagia is clinically defined as losing more than 80 milliliters of blood per cycle or having periods lasting longer than seven days. But you don’t need to measure—if bleeding interferes with your daily activities, it’s too heavy.
The location of the fibroids matters more than size when predicting bleeding severity. A small submucosal fibroid protruding into the uterine cavity often causes worse bleeding than a large intramural fibroid buried in the uterine wall.
Treatment should be tailored to:
Your symptoms and their severity
The size, number, and location of fibroids
Your age and desire for future pregnancy
Your overall health and treatment preferences
Dr. Samir Abdel Ghaffar offers comprehensive evaluation and treatment planning. As a consultant in interventional radiology, he specializes in catheter-based treatments that provide relief without the risks and recovery time of traditional surgery.
Frequently Asked Questions
Why do fibroids cause large blood clots?
Large blood clots form when bleeding is so heavy that blood pools in the uterus before being expelled. Fibroids in the uterine cavity are particularly prone to causing this because they create a reservoir where blood can collect and clot. The body’s natural anticoagulants can’t keep up with the volume, resulting in clots that can be alarmingly large.
Can tranexamic acid treat fibroids?
Tranexamic acid doesn’t treat fibroids themselves—it treats the symptom of heavy bleeding. This medication works by preventing blood clots from breaking down too quickly, which reduces menstrual blood loss. Many women find it helpful for managing heavy periods while deciding on definitive fibroid treatment. However, it’s a temporary solution, not a cure for fibroids.
Why am I passing very large blood clots?
Very large blood clots during your period usually indicate excessive menstrual bleeding. When blood flow exceeds your body’s ability to prevent clotting, blood pools and forms clots before being expelled. Fibroids are a common cause, but other conditions like adenomyosis, bleeding disorders, or hormonal imbalances can also be responsible. Any clots larger than a quarter warrant medical evaluation.
When is fibroid bleeding an emergency?
Seek emergency care if you’re soaking through a pad or tampon every hour for more than two hours, passing clots larger than a golf ball, experiencing severe pain, feeling faint or dizzy, or having chest pain or difficulty breathing. These symptoms suggest dangerous blood loss that could lead to severe anemia or other complications requiring immediate intervention.
Why do I pass golf ball sized blood clots during my period?
Golf ball sized clots indicate very heavy menstrual bleeding, often from fibroids that have significantly increased your uterine cavity size or disrupted normal uterine contractions. This level of bleeding isn’t normal and puts you at risk for severe anemia. You should contact your doctor promptly to discuss treatment options that can reduce this excessive bleeding.
Take Control of Your Health Today
Living with heavy bleeding and large clots doesn’t have to be your reality. Understanding why fibroids cause these symptoms empowers you to make informed decisions about treatment.
Uterine artery embolization offers a proven alternative to hysterectomy, preserving your uterus while effectively reducing bleeding and other fibroid symptoms. With over 90% of women experiencing significant symptom improvement, UAE represents a safe, effective path to reclaiming your life. ✨
Contact Dr. Samir Abdel Ghaffar for expert consultation:
London, UK:
Clinic: 00442081442266
WhatsApp: 00447377790644
Egypt:
Cairo Booking: +201000881336
WhatsApp: +201000881336
Don’t let fibroids control your life. Schedule your consultation today and discover how minimally invasive treatment can help you feel like yourself again.
Are you experiencing unpredictable periods that arrive too early, too late, or with flooding that disrupts your daily life? You’re not alone in wondering about fibroids.
Month after month, the uncertainty builds. You can’t plan vacations, important meetings, or even a simple night out without fear of unexpected bleeding. The cramping intensifies, the flow becomes heavier, and you’re left wondering what’s happening inside your body.
You can regain control by understanding the truth about does fibroids cause irregular periods?
Many women blame stress or age when their periods become erratic, but the truth might lie deeper—literally. When tissues in the uterus develop abnormal growths, they can completely disrupt your normal menstrual patterns. These benign muscle growths affect approximately 70% of women by age 50, with many women aged 30-40 having uterine fibroids without even knowing it.
The connection between these growths and menstrual irregularities isn’t just about timing. The location of uterine fibroids plays a crucial role in determining which symptoms you’ll experience and how severely they’ll impact your reproductive health.
Does Fibroids Cause Irregular Periods?
Yes, fibroids can absolutely cause irregular periods, but the relationship is more complex than you might think.
Fibroids don’t affect everyone the same way. Some women with large growths experience perfectly regular cycles, while others with smaller ones face significant disruptions. What matters most is where these benign tumors develop and how they interact with your uterine lining.
When fibroids grow inside the uterine cavity or just beneath the lining (submucosal fibroids), they create a larger surface area that needs to shed during menstruation. This leads to heavier, more prolonged bleeding that can last well beyond your typical period length. The irregular patterns emerge because:
The endometrial tissue stretches over fibroid surfaces unevenly
Hormone balance shifts as fibroids respond to estrogen levels
Blood vessels around growths become enlarged and fragile
The uterus struggles to contract effectively during your cycle
Research shows that women aged 30-40 have uterine fibroids at rates between 20-40%, with many experiencing menstrual changes as their first symptom. The size, location, and number of growths all determine whether your periods become shorter, longer, heavier, or completely unpredictable.
Understanding this connection helps you recognize that irregular cycles aren’t just “bad luck”—they’re often your body signaling that something needs attention.
What Happens to Fibroids When Periods Stop?
The transition into menopause brings significant changes for fibroid sufferers, mostly positive ones.
As you approach perimenopause and menopause, your estrogen levels naturally decline. Since fibroids depend heavily on estrogen to maintain their size and growth, this hormonal shift typically causes them to shrink. Many women find relief from symptoms including heavy bleeding, pelvic pressure, and painful cramps during this transition.
However, the journey isn’t always smooth:
During perimenopause, your hormone levels fluctuate wildly. Some months you produce more estrogen than others, which can temporarily enlarge fibroids and cause unpredictable bleeding patterns. This phase can be particularly unsettling because you might experience:
Spotting between irregular cycles
Sudden heavy bleeding after months of lighter flow
Prolonged periods that seem endless
Brown discharge as older blood is expelled
After menopause, when periods stop completely and estrogen production drops significantly, most fibroids shrink to a fraction of their original size. Women who suffered for years often find their symptoms disappear without any medical intervention.
There’s an important exception though: if you’re taking hormone replacement therapy (HRT) for menopausal symptoms, the synthetic hormones might prevent fibroids from shrinking naturally. Your doctor needs to balance your quality of life against fibroid management when determining the best treatment approach.
Can Fibroids Cause 2 Week Periods?
Absolutely, and it’s one of the most common complaints among women with submucosal or intramural fibroids.
Your typical menstrual cycle should last between 3-7 days. When periods extend to two weeks or longer, it’s called prolonged menstrual bleeding, and fibroids are among the leading causes.
Here’s what’s happening inside your uterus:
The normal menstruation process involves your uterine lining building up, then shedding when pregnancy doesn’t occur. This usually happens efficiently over a few days. But when fibroids are present:
The enlarged uterine cavity takes longer to completely shed its lining
Fibroids disrupt the uterus’s ability to contract and stop bleeding
Blood vessels around growths continue releasing blood even after normal flow should end
The endometrial tissue grows unevenly, shedding in waves rather than all at once
Women with 2-week periods often experience phases within their prolonged bleeding:
Heavy flow for the first 5-7 days
Moderate bleeding for another 3-4 days
Light spotting or brown discharge for the remaining time
This pattern differs from normal cycles and typically indicates that fibroids are affecting the uterine cavity’s ability to function properly. The constant bleeding isn’t just inconvenient—it can lead to iron deficiency, fatigue, and anemia if left unaddressed.
If your periods consistently last beyond 10 days, it’s time to seek medical evaluation to determine the underlying cause and explore treatment options.
Can Fibroids Kill You?
Let’s address this fear directly: fibroids themselves are benign growths that won’t kill you, but complications from untreated fibroids can become serious.
The reality is that uterine fibroids are non-cancerous. The chance of a fibroid being cancerous (leiomyosarcoma) is extremely rare—less than 1 in 1,000 cases. However, ignoring severe symptoms can lead to life-threatening conditions:
Severe anemia develops when prolonged, heavy bleeding depletes your iron stores faster than you can replace them. Symptoms include:
Extreme fatigue that doesn’t improve with rest
Shortness of breath during normal activities
Rapid heartbeat and chest pain
Pale skin and cold hands
Without treatment, severe anemia can strain your heart and require emergency blood transfusions.
Acute fibroid degeneration happens when a fibroid outgrows its blood supply and begins to die. This causes:
Sudden, intense pelvic pain
Fever and infection risk
Potential sepsis if bacteria enter the dying tissue
Reproductive complications matter too. Large fibroids can pressure nearby organs, blocking the ureters (tubes from kidneys to bladder) and potentially causing kidney damage if blood flow becomes restricted.
The key message? Fibroids won’t kill you, but their complications require medical attention. Regular monitoring and appropriate treatment prevent these serious outcomes entirely.
How to Get Rid of Uterine Fibroids
You have more options than ever before, and surgery isn’t always necessary. 💡
Traditional approaches focused on invasive procedures, but modern medicine offers several effective treatment paths depending on your symptoms, age, and future pregnancy plans:
Medication approaches work well for managing symptoms:
Hormonal birth control regulates bleeding patterns
These options don’t eliminate fibroids but can make symptoms manageable, especially if you’re approaching menopause.
Minimally invasive procedures include:
Uterine artery embolization (UAE) stands out as a game-changing option. This catheterization procedure, performed by interventional radiologists like Dr. Samir Abdel Ghaffar, blocks blood flow to fibroids, causing them to shrink dramatically without surgery. The benefits include:
No surgical incision required
Preserve your uterus completely
Treat multiple fibroids simultaneously
Quick recovery—most women return to normal activities within a week
Effective for 85-90% of women
MRI-guided focused ultrasound uses heat to destroy fibroid tissue without incisions.
Surgical options remain available when other treatments fail:
Myomectomy removes fibroids while preserving the uterus
Hysterectomy removes the entire uterus (most invasive option)
The best approach depends on your individual circumstances. Understanding these options empowers you to choose the treatment that aligns with your health goals and lifestyle.
Signs of Fibroids Breaking Down
Fibroid degeneration occurs when growths outpace their blood supply and begin dying—a process that comes with distinct symptoms.
This breakdown typically happens when fibroids grow rapidly during pregnancy or when blood flow is intentionally cut off during procedures like uterine artery embolization. Recognizing the signs helps you distinguish normal post-treatment changes from complications requiring urgent care.
Common symptoms of fibroid degeneration include:
Sharp, sudden pelvic pain that feels different from menstrual cramps
Fever ranging from low-grade to high (above 100.4°F)
Nausea and vomiting
Increased vaginal discharge
Feeling pressure or fullness in your lower abdomen
The pain pattern matters. Degeneration pain usually:
Starts suddenly rather than gradually building
Localizes to one specific area where the fibroid is located
Intensifies over several hours to days
Doesn’t respond well to over-the-counter pain relievers initially
Different types of degeneration create varying symptoms:
Hyaline degeneration (most common) causes fibroids to soften and may produce mild discomfort. Red degeneration, more common during pregnancy, involves bleeding into the fibroid and causes severe pain requiring medical evaluation.
After planned procedures like UAE, some degeneration is expected and actually indicates the treatment is working. Your doctor will explain what’s normal versus what requires immediate attention.
If you experience sudden severe pain with fever, don’t wait—seek medical care to rule out infection or other complications.
Fibroids Period Symptoms
Period symptoms with fibroids go far beyond just heavy bleeding, creating a constellation of issues that affect your quality of life. 🩸
Heavy menstrual bleeding tops the list. You might notice:
Soaking through pads or tampons every hour
Needing to change protection during the night
Passing large blood clots (bigger than a quarter)
Bleeding that lasts longer than 7 days
Painful cramps intensify because your uterus works harder to expel blood around fibroids. The pain often feels like:
Severe cramping in your lower abdomen
Pressure extending to your lower back
Sharp pains that radiate down your thighs
Constant aching that doesn’t ease between contractions
Irregular bleeding patterns manifest as:
Periods arriving earlier or later than expected
Spotting between cycles
Brown discharge before or after your period
Unpredictable cycle lengths month to month
Fatigue and weakness develop from anemia caused by excessive blood loss. You’ll experience:
Exhaustion that sleep doesn’t fix
Difficulty concentrating at work
Dizziness when standing quickly
Pale complexion and brittle nails
Pelvic pressure creates a sensation of fullness or heaviness that worsens during menstruation. Some women describe it as feeling like something is “falling out” or constant pressure on their bladder.
These symptoms don’t just appear during your period. Many women with fibroids experience pelvic discomfort, frequent urination, and constipation throughout their entire cycle, with symptoms intensifying during menstruation.
Tracking your symptoms helps your healthcare provider determine the best treatment approach tailored to your specific fibroid-related challenges.
Can Fibroid Stop Pregnancy?
Fibroids can affect your ability to conceive and maintain a healthy pregnancy, but the impact varies dramatically based on location and size.
The good news? Most women with fibroids can still get pregnant and deliver healthy babies. Studies show that only 5-10% of infertility cases are directly caused by fibroids alone. However, certain types create more obstacles than others.
How fibroids interfere with pregnancy:
Conception challenges arise when:
Submucosal fibroids distort the uterine cavity, preventing embryo implantation
Large fibroids block fallopian tubes, stopping sperm from reaching eggs
Growths alter the uterine lining’s ability to support a fertilized egg
Higher miscarriage rates, especially with submucosal fibroids
Placental problems if fibroids compete for blood supply
Preterm labor triggered by limited space for baby growth
Abnormal fetal positioning (breech presentation)
Increased cesarean section rates
Location matters most:
Submucosal fibroids (growing into the uterine cavity) cause the most reproductive issues. Intramural fibroids (within the uterine wall) can interfere if they’re large or numerous. Subserosal fibroids (growing outward) rarely affect fertility unless they’re massive.
Treatment timing is crucial:
If you’re planning pregnancy, discuss treatment with specialists. Myomectomy can remove fibroids while preserving fertility, but the uterus needs 3-6 months to heal before conception. Uterine artery embolization effectiveness for future pregnancy remains debated, though many women have conceived successfully afterward.
The key is getting evaluated before trying to conceive. Understanding your fibroid situation lets you make informed decisions about treatment timing and pregnancy planning.
Understanding the Location of Uterine Fibroids
Where your fibroids grow determines everything about your experience—from symptoms to treatment success.
Fibroids develop in three primary locations, each creating distinct challenges:
Submucosal fibroids grow just beneath the uterine lining, protruding into the cavity. These cause the most severe menstrual symptoms:
Extremely heavy bleeding during periods
Prolonged menstrual cycles
Difficulty with pregnancy implantation
Higher risk of infertility
Even small submucosal fibroids can disrupt your cycle significantly because they directly interfere with the endometrial lining’s normal function.
Intramural fibroids develop within the muscular uterine wall—the most common type. Their symptoms depend on size:
Mild cases may produce no symptoms
Larger growths cause pelvic pressure and frequent urination
Very large intramural fibroids can distort the uterine shape
May cause both heavy bleeding and bulk symptoms
Subserosal fibroids grow outward from the uterus’s outer wall. These rarely affect menstrual bleeding but create pressure symptoms:
Backache and leg pain
Constipation from rectal pressure
Frequent urination from bladder compression
Visible abdominal enlargement with very large growths
Pedunculated fibroids attach to the uterus by a stalk and can be either submucosal or subserosal. These sometimes twist on their stalk, causing sudden severe pain requiring emergency treatment.
Understanding your fibroid location helps determine which treatment approaches will work best. For example, hysteroscopic removal works excellently for submucosal fibroids, while uterine artery embolization effectively treats all fibroid types regardless of location.
Dr. Samir Abdel Ghaffar uses advanced imaging to precisely map fibroid locations before recommending treatment, ensuring the most effective approach for your specific situation.
Common Causes of Irregular Periods Beyond Fibroids
While fibroids frequently cause menstrual irregularities, other conditions can create similar symptoms—making accurate diagnosis essential.
Uterine polyps
Uterine polyps are small, benign growths in the uterine lining that cause:
Spotting between periods
Heavy menstrual bleeding
Irregular cycle timing
Bleeding after menopause
Unlike fibroids, polyps are softer and usually smaller. They’re easily removed during hysteroscopy.
Adenomyosis
Adenomyosis occurs when endometrial tissue grows into the uterine muscle wall. Symptoms include:
Severely painful periods
Heavy prolonged bleeding
Enlarged, tender uterus
Pain during intercourse
This condition often coexists with fibroids, complicating diagnosis and treatment.
Polycystic ovary syndrome
Polycystic ovary syndrome (PCOS) disrupts hormone balance, leading to:
Missed or skipped periods
Very irregular cycle timing
Difficulty predicting ovulation
Other hormonal symptoms like acne and excess hair growth
Thyroid disorders
Thyroid disorders affect every body system, including your reproductive cycle:
Hypothyroidism can cause heavier, longer periods
Hyperthyroidism typically creates lighter, shorter cycles
Both conditions disrupt cycle regularity
Pelvic inflammatory disease
Pelvic inflammatory disease (PID), an infection of reproductive organs, causes:
Irregular bleeding
Pelvic pain
Fever and abnormal discharge
Potential fertility problems if untreated
Perimenopause
Perimenopause represents the natural transition toward menopause, characterized by:
Wildly fluctuating hormone levels
Unpredictable cycle lengths
Skipped periods alternating with heavy ones
Gradually decreasing fertility
Stress and lifestyle factors
Stress and lifestyle factors shouldn’t be overlooked:
Extreme weight changes
Excessive exercise
Chronic stress
Poor nutrition
These factors can temporarily disrupt your hormonal balance and menstrual patterns.
Endometrial cancer
Endometrial cancer is rare but serious. Warning signs include:
Postmenopausal bleeding
Abnormally heavy periods after age 40
Bleeding between periods
Pelvic pain
Accurate diagnosis requires proper medical evaluation. Blood tests, ultrasound, MRI, and sometimes hysteroscopy help distinguish between these conditions and fibroids, ensuring you receive appropriate treatment.
Frequently Asked Questions
Can fibroids affect menstruation?
Yes, fibroids significantly affect menstruation in most women who have symptoms. The impact depends on fibroid size, number, and especially location. Submucosal fibroids that grow into the uterine cavity create the most dramatic menstrual changes, including heavy bleeding, prolonged periods, and irregular timing. Even women without noticeable symptoms may experience subtle cycle changes as fibroids develop.
What are the signs of fibroids in a woman?
Common signs include heavy menstrual bleeding with large clots, periods lasting longer than 7 days, pelvic pressure or pain, frequent urination, constipation, backache, and an enlarged abdomen. Many women also experience pain during intercourse, difficulty emptying the bladder completely, and leg pain if fibroids press on nerves. Some women have no symptoms at all, discovering fibroids only during routine pelvic exams or pregnancy ultrasounds.
How to treat fibroids during pregnancy?
Treatment during pregnancy is conservative because most procedures risk harming the baby. Doctors typically monitor fibroids with ultrasound and manage symptoms with:
Safe pain medications like acetaminophen
Bed rest during painful episodes
Increased hydration
Close monitoring for complications
Most fibroids don’t grow significantly during pregnancy. Surgical intervention is reserved for rare emergencies like fibroid torsion or severe degeneration.
Can tranexamic acid treat fibroids?
Tranexamic acid doesn’t treat or shrink fibroids themselves, but it effectively reduces heavy menstrual bleeding caused by fibroids. This medication helps blood clot more effectively, reducing flow by 40-50% in many women. It’s taken only during your period, making it a good option for managing symptoms while you decide on definitive treatment or if you’re not a candidate for procedures.
How does fibroid menstruation look like?
Fibroid-affected periods typically involve very heavy flow with bright red blood in the beginning, progressing to darker blood later. You’ll likely pass large, gel-like blood clots—sometimes golf-ball sized or larger. The bleeding often soaks through protection within an hour or two during peak days. Many women notice prolonged bleeding that continues as brown or pink spotting well beyond their normal period length. 🔴
What are the main causes of irregular periods?
The main causes include hormonal imbalances from thyroid disorders or PCOS, uterine abnormalities like fibroids and polyps, stress and significant weight changes, perimenopause, certain medications including blood thinners, chronic health conditions affecting hormone levels, excessive exercise, and reproductive system infections like PID. Age also plays a role—periods naturally become more irregular as women approach menopause.
What happens if fibroids are left untreated?
Untreated fibroids may continue growing, worsening symptoms over time. Potential complications include severe anemia from chronic blood loss, fertility problems or pregnancy complications, chronic pelvic pain affecting quality of life, urinary problems from bladder compression, and rarely, kidney damage if ureters become blocked. However, many small fibroids remain stable for years without causing problems. The decision to treat depends on symptom severity and impact on daily life.
What is the fastest way to shrink fibroids?
Uterine artery embolization (UAE) offers the fastest significant shrinkage, with fibroids typically reducing 40-60% in size within 3-6 months. This minimally invasive procedure blocks blood flow to fibroids, causing them to shrink and symptoms to improve rapidly.
GnRH agonists create temporary shrinkage within weeks but come with significant side effects and aren’t long-term solutions. Natural menopause also shrinks fibroids as estrogen levels drop, but this takes years. No diet, supplement, or exercise program has proven to rapidly shrink fibroids, despite many online claims.
Take Control of Your Health Today
You don’t have to live with the disruption, pain, and uncertainty that fibroids bring to your menstrual cycle.
Understanding the connection between fibroids and irregular periods is your first step, but taking action creates real change. Modern treatment options—especially minimally invasive procedures like uterine artery embolization—offer effective relief without the risks and recovery time of traditional surgery.
Dr. Samir Abdel Ghaffar specializes in treating uterine fibroids through advanced interventional radiology techniques. With years of expert experience in catheterization procedures, he offers a safe alternative to hysterectomy that preserves your uterus while effectively addressing fibroid symptoms.
Whether you’re experiencing heavy bleeding, prolonged periods, pelvic pressure, or fertility concerns, professional evaluation determines the underlying cause and maps the best treatment path for your unique situation.
Ready to reclaim your life from fibroid symptoms?
Contact Dr. Samir Abdel Ghaffar:
In London, UK:
Clinic: 00442081442266
WhatsApp: 00447377790644
In Cairo, Egypt:
Booking: +201000881336
WhatsApp: +201000881336
Your journey toward regular, manageable periods and improved quality of life starts with one conversation. Don’t wait for symptoms to worsen—explore your options today.
You’ve been told you have subserosal fibroids, and suddenly you’re facing uncomfortable symptoms, concerns about fertility, and the scary prospect of major surgery.
The pressure in your pelvic area keeps growing, your clothes feel tighter, and you worry whether these benign tumors will affect your chances of having children or require removing your uterus entirely.
What if there was a way to treat subserosal uterine fibroids without going under the knife? Modern medicine offers minimally invasive approaches that preserve your uterus while delivering effective treatment and improved quality of life.
Understanding your options for subserosal uterine fibroid treatment starts with knowing exactly what you’re dealing with and why location matters when it comes to these common growths.
What Are Subserosal Uterine Fibroids and Why Does Location Matter?
Subserosal uterine fibroids are noncancerous tumors that develop on the outer wall of your uterus. Unlike their cousins—intramural fibroids that grow within the uterine muscle wall or submucosal fibroids that project into the uterine cavity—subserosal fibroids grow outward from the surface of the uterus.
Think of your uterus as having three layers. Subserosal fibroids are classified based on their location on the outermost layer. According to the FIGO classification system used by medical professionals worldwide, these growths can remain attached to the uterine wall or develop on a stalk (called pedunculated subserosal fibroids).
The location of these benign tumors significantly affects what symptoms you might experience and which treatment approaches work best. Because they grow toward the outside rather than inward, many women with subserosal leiomyomas remain asymptomatic for years. However, as these smooth muscle tumors grow larger, they can press against nearby organs, causing distinct discomfort.
Understanding the type of fibroid you have helps both you and your doctor explore the most appropriate management options tailored to your specific situation.
Subserosal Uterine Fibroid Symptoms: What Should You Watch For?
While some women feel absolutely nothing, others experience symptoms that affect their daily life. The key difference with subserosal fibroids compared to other types is that they typically don’t cause heavy bleeding or abnormal menstrual periods since they’re located on the outer surface rather than inside the uterine cavity.
Common symptoms include:
Pelvic pressure or fullness that feels like something is pushing against your bladder or bowel
Bloating that makes your abdomen appear larger, especially as fibroids grow
Lower back pain when larger tumors press against nerves or muscles
Frequent urination if the fibroid presses on your bladder
Constipation when growths push against your bowels
Pain during intercourse depending on fibroid location
Discomfort when lying face down or in certain positions
The symptoms you experience depend largely on how big the fibroid has grown and exactly where it’s located. A small subserosal fibroid might cause zero problems, while a larger one pressing against your bladder could send you running to the bathroom every hour.
During perimenopause, when hormone levels fluctuate, some women notice their fibroids growing faster, which can intensify these symptoms.
Subserosal Pedunculated Fibroid: A Special Type Worth Understanding
Pedunculated subserosal fibroids deserve special attention because they behave differently from their broad-based counterparts. These particular fibroids grow on a stalk extending from the uterine wall, somewhat like a mushroom on a stem.
This type of growth pattern creates unique considerations:
Movement and twisting: Because they’re attached by a narrow stalk, pedunculated fibroids can sometimes twist on themselves, cutting off their blood supply. This causes sudden, severe pain that requires immediate medical care.
Diagnostic challenges: During examination or imaging, pedunculated fibroids can sometimes be mistaken for ovarian masses because they may sit away from the uterus itself.
Treatment implications: The stalk attachment affects which surgical approaches work best if intervention becomes necessary. Some pedunculated fibroids are easier to remove than broad-based ones, while others require careful planning.
Symptom variability: Depending on where the stalk positions the fibroid, you might feel pressure in different areas as you move or change positions throughout the day.
If imaging reveals you have a pedunculated subserosal fibroid, your doctor will likely monitor it more closely and discuss management strategies based on its size and whether it’s causing symptoms.
Subserosal Fibroid and Fertility: Will It Affect Your Chances of Pregnancy?
This question weighs heavily on many women, and the answer offers more hope than you might expect. 💚
Subserosal fibroids generally have less impact on fertility compared to submucosal fibroids because they don’t distort the uterine cavity where a baby would implant and grow. However, several factors influence fertility outcomes:
Size matters: Larger subserosal fibroids may create pressure that affects the normal shape of your uterus or blocks the fallopian tubes, potentially impacting pregnancy possibilities.
Location is crucial: A subserosal fibroid near the opening of your fallopian tubes could interfere with the egg’s journey, while one located elsewhere might have no effect at all.
Multiple vs. single: Women with numerous fibroids throughout the uterus face different considerations than those with a single subserosal growth.
Research shows that most women with subserosal fibroids can conceive naturally. A particular study examining fertility outcomes in women who underwent uterine artery embolization found encouraging results, with many patients achieving successful pregnancies after this minimally invasive procedure.
The key is finding the right balance between treating bothersome symptoms and preserving your reproductive potential. Modern treatment options allow you to address problematic fibroids while keeping future pregnancy possibilities open.
Subserosal Fibroid Location: Why It Determines Your Treatment Path
Not all subserosal fibroids are created equal, and their exact location on the outer uterine wall plays a huge role in determining the best treatment approach.
Anterior location (front of the uterus): These often press on the bladder, causing frequent urination. They’re typically easier to access during certain procedures.
Posterior location (back of the uterus): Fibroids here may cause lower back pain or constipation as they push against the bowel. They can be trickier to reach with some surgical approaches.
Fundal location (top of the uterus): Growing near the top, these fibroids might cause upper abdominal pressure or bloating.
Lateral location (sides near ovaries): These can sometimes affect the fallopian tubes or be confused with ovarian masses during diagnosis.
The FIGO classification system helps doctors categorize these locations precisely, ensuring everyone on your care team understands exactly what they’re dealing with. This standardized approach improves outcomes by helping specialists plan the most effective treatment strategy based on comprehensive understanding of your specific situation.
What Is Considered a Large Subserosal Fibroid?
Fibroids are measured in centimeters, and what counts as “large” might surprise you.
Small fibroids: Less than 5 cm (about the size of a plum) Medium fibroids: 5-10 cm (similar to an orange or grapefruit) Large fibroids: Greater than 10 cm (comparable to a melon or larger)
Some subserosal fibroids grow to truly remarkable sizes—reports exist of fibroids weighing several pounds. Generally, anything over 10 centimeters is considered large and more likely to cause symptoms simply due to the space it occupies in your pelvic area.
Size affects treatment decisions because:
Larger fibroids may require different approaches than smaller ones
They’re more likely to cause compression symptoms affecting nearby organs
Post-procedure recovery might vary based on fibroid size
Some treatments work better on specific size ranges
However, size alone doesn’t determine whether you need treatment. A large asymptomatic fibroid might simply need monitoring, while a smaller symptomatic one could warrant intervention. Your doctor considers the complete picture—size, location, symptoms, and your personal goals—when recommending management options.
Subserosal Fibroid and Pregnancy: What to Expect
If you’re pregnant and have subserosal fibroids, or you’re planning to conceive, understanding how these growths interact with pregnancy helps set realistic expectations.
During pregnancy:
Most subserosal fibroids don’t cause pregnancy complications. The growing uterus often accommodates these external growths without issue. However, larger fibroids may:
Increase the risk of cesarean delivery if they block the birth canal
Cause more pelvic pain as your uterus expands
Rarely, undergo “red degeneration” (when they outgrow their blood supply), causing significant pain that usually resolves with conservative care
Effect on the baby:
Subserosal fibroids typically don’t affect fetal development because they grow outward rather than into the space where your baby develops. Submucosal fibroids pose greater risks to pregnancy than subserosal ones.
Pregnancy after treatment:
Women who undergo uterine fibroid embolization can often conceive afterward, though a retrospective study suggests waiting several months to allow complete healing. This minimally invasive procedure preserves the uterus while treating problematic fibroids, making it an attractive option for women concerned about post-procedure fertility.
Your reproductive goals should guide treatment decisions. Open conversations with your healthcare provider about timing, risks, and the various approaches available ensure you make informed choices that align with your life plans.
Subserosal Fibroid Cancer: Should You Worry?
Let’s address the elephant in the room: Could your subserosal fibroid actually be cancerous?
The short answer is that it’s extremely unlikely. Uterine fibroids—also called leiomyomas or myomas—are benign growths, meaning they’re not cancerous. The transformation of a benign fibroid into a leiomyosarcoma (cancerous smooth muscle tumor) is exceptionally rare, occurring in less than 1% of cases.
Signs that warrant further investigation:
Unusual pain patterns
Unexpected bleeding
Rapid growth, especially after menopause
Growing fibroids despite medications that should stabilize them
Your doctor uses imaging and sometimes additional tests to distinguish benign fibroids from the rare cancerous growth. MRI scans can often identify suspicious features that differ from typical benign leiomyomas.
While cancer risk is minimal, regular monitoring of known fibroids makes sense, particularly if they’re growing or changing. This vigilance isn’t about living in fear—it’s about staying informed and catching the rare exception early if it occurs.
For the vast majority of women, subserosal fibroids remain benign throughout life and pose no cancer risk whatsoever.
Is Subserosal Fibroid Dangerous? Understanding Real Risks
Subserosal fibroids themselves aren’t dangerous in most cases, but complications can develop that require attention.
Actual risks to consider:
Torsion of pedunculated fibroids: When a fibroid on a stalk twists, it can cut off blood supply, causing severe pain and requiring emergency care.
Compression effects: Very large fibroids pressing on organs can affect bladder or bowel function, though this rarely causes permanent damage.
Quality of life impact: Chronic pain, bloating, and discomfort significantly affect your daily activities and emotional well-being, even if not “medically dangerous.”
Rare complications: In exceptional cases, very large fibroids can cause anemia (not from bleeding, but from stealing blood supply from normal tissues) or kidney problems if they compress the ureters.
What’s NOT a significant danger:
They won’t “spread” like cancer
They don’t typically cause life-threatening bleeding
Most don’t interfere with vital organ function
The main concern with subserosal fibroids is how they affect your life quality rather than posing immediate health dangers. That said, any fibroid causing significant symptoms deserves treatment—you shouldn’t have to live with constant discomfort just because something isn’t technically “dangerous.”
subserosal uterine fibroid treatment: Exploring Your Options Beyond Surgery
Here’s where things get interesting. You have more choices than you might think, and understanding each option helps you make decisions that fit your life.
Watchful waiting: If your fibroids aren’t causing symptoms, monitoring them with periodic imaging might be the best approach. Many subserosal fibroids remain stable for years.
Medications: Hormonal medications can help manage symptoms, though they don’t eliminate fibroids. Options include birth control pills, GnRH agonists, and newer medications that target specific receptors. Some patients explore complementary approaches like Crinum latifolium dry extract or EGCG (from green tea), though evidence for these remains limited.
Uterine artery embolization (UAE): This minimally invasive procedure offers effective treatment without removing your uterus. Dr. Samir Abdel Ghaffar specializes in this approach, which involves blocking blood flow to fibroids through catheterization, causing them to shrink. Recovery takes days rather than weeks, and the uterus remains intact—a crucial consideration for women concerned about fertility or who simply want to keep their reproductive organs.
Myomectomy: Surgical removal of fibroids while preserving the uterus. For subserosal fibroids, this can often be done laparoscopically (through small incisions) rather than open surgery.
Hysterectomy: Complete uterine removal—a definitive solution but one that ends fertility and carries the psychological and physical impacts of losing an organ.
The best treatment depends on your symptoms, fibroid characteristics, reproductive plans, and personal preferences. Minimally invasive options like uterine artery embolization have revolutionized care, offering relief without the complications associated with major surgery.
Frequently Asked Questions
How serious is subserosal fibroid?
Most subserosal fibroids aren’t medically serious, though they can significantly impact your quality of life through pain, pressure, and bloating. The seriousness depends on size, location, symptoms, and whether complications develop. Large fibroids or those causing severe symptoms warrant treatment, but they’re rarely life-threatening.
Are subserosal fibroids easy to remove?
Subserosal fibroids located on the outer uterine surface are often easier to remove surgically compared to intramural types embedded within the uterine wall. Pedunculated subserosal fibroids on a stalk can sometimes be removed quite easily. However, “easy” is relative—any surgical procedure carries risks and recovery time. Minimally invasive alternatives like uterine artery embolization avoid removal altogether by shrinking the fibroid.
How to reduce subserosal fibroids?
Several approaches can reduce fibroid size: uterine fibroid embolization cuts off blood supply, causing shrinkage over several months; certain medications temporarily reduce size; and some lifestyle modifications (maintaining healthy weight, anti-inflammatory diet) may slow growth. Natural compounds like EGCG are being studied, though results remain preliminary. The most reliable reduction comes from medical interventions rather than natural methods alone.
What is the normal size of a subserosal fibroid?
There’s no “normal” size for fibroids—they range from microscopic to enormous. However, fibroids under 5 cm are considered small, those between 5-10 cm are medium, and anything over 10 cm is large. Many women have small subserosal fibroids that never cause problems and never grow significantly.
When should subserosal fibroids be removed?
Consider removal or treatment when fibroids cause bothersome symptoms affecting your daily life, grow rapidly, cause fertility concerns, or develop complications. Asymptomatic fibroids usually just need monitoring. The decision should be based on how the fibroid impacts you personally rather than size or presence alone.
How do you get rid of subserosal fibroids without surgery?
Uterine artery embolization provides effective treatment through a catheter-based procedure that requires no incisions. This approach blocks blood flow to fibroids, causing them to shrink while preserving the uterus. Other non-surgical options include MRI-guided focused ultrasound (though less common) and certain medications that temporarily shrink fibroids. These minimally invasive alternatives offer relief without the recovery time and risks associated with surgical removal.
What is the best treatment for uterine fibroids?
The “best” treatment varies by individual. For women wanting to preserve fertility and avoid major surgery, uterine artery embolization offers an excellent balance of effectiveness and minimal invasiveness. Studies show good outcomes with this approach, including acceptable fertility results and significant symptom relief. The best treatment is the one that addresses your specific symptoms, aligns with your reproductive goals, and fits your lifestyle—making individualized care essential rather than a one-size-fits-all approach.
Finding Relief: Your Path Forward with Expert Care
Living with subserosal fibroids doesn’t mean accepting discomfort or facing surgery as your only option. Understanding the different types of uterine fibroids, how they’re classified, and what treatment approaches exist empowers you to make informed decisions about your health.
Modern medicine offers alternatives to traditional surgical interventions. Uterine artery embolization represents a significant advancement in fibroid care—a minimally invasive procedure that delivers effective treatment while preserving your uterus and maintaining pregnancy possibilities for those who desire future children.
Dr. Samir Abdel Ghaffar, a consultant in interventional radiology, specializes in treating uterine fibroids through catheterization without surgery. His expertise in this technique has helped numerous patients find relief from symptomatic fibroids while avoiding the complications and extended recovery associated with hysterectomy or surgical myomectomy.
Whether you’re dealing with pelvic pressure, bloating, or concerns about fertility, comprehensive diagnosis and expert management can significantly improve your quality of life. The key is finding a specialist who understands the nuances of fibroid location, growth patterns, and how different treatment approaches affect long-term outcomes.
Don’t let subserosal fibroids control your life. Modern interventional radiology techniques offer safe, effective alternatives to major surgery, with improved recovery times and excellent results.
Contact Dr. Samir Abdel Ghaffar for Expert Fibroid Treatment ✨
Ready to explore minimally invasive treatment options for your subserosal uterine fibroids?
Take the first step toward relief today. Your journey to better health and comfort starts with understanding your options and connecting with specialists who offer proven alternatives to traditional surgery.
Do you feel a heaviness in your pelvis or notice your clothes fitting tighter, yet you aren’t gaining weight elsewhere? You might have been diagnosed with a fibroid and are now panicking about the numbers on your ultrasound report. Worrying about which size of fibroid is normal is a common reaction, but you don’t have to navigate this fear alone. Here, we break down the sizes, risks, and how to treat them without surgery.
Which Size of Fibroid Is Normal? (The Short Answer)
When patients ask which size of fibroid is normal, the medical answer is slightly nuanced. Anatomically, a “normal” uterus should not have any fibroids at all. However, because Uterine fibroids are so incredibly common among women of reproductive age, having small, asymptomatic fibroids is often considered “clinically normal” or manageable.
Generally, Smaller fibroids that are less than 1 cm to 5 cm (about the size of a seed to a lime) are frequently viewed as “normal” or harmless if they aren’t causing symptoms. There isn’t a single “cutoff” number where a fibroid switches from normal to abnormal; rather, it is about how the fibroid size impacts your life. A 2 cm fibroid inside the uterine cavity might cause severe bleeding, while a 6 cm fibroid on the outer wall might be completely silent.
In this guide, we will explore the average uterine fibroid size ranges, helping you understand when to watch and wait, and when to seek the expertise of Dr. Samir Abdel Ghaffar for non-surgical catheterization.
Understanding the Muscular Wall of the Uterus and Growth
Fibroids are noncancerous growths that develop in or on the muscular wall of the uterus. They can be singular or multiple, and their growth patterns are unpredictable. Some remain the same size for years, while others grow rapidly.
Understanding the location is just as crucial as the size.
Subserosal: Grow on the outside.
Intramural: Grow within the wall.
Submucosal: Grow inside the cavity (these often cause the most issues even at small sizes).
Hormones like estrogen and progesterone fuel their growth, which is why they often affect women during their reproductive years and may shrink after menopause.
Fibroid Sizes Chart: From Seed to Watermelon
To help you visualize the size of the fibroids, we use fruit analogies. This helps in understanding the medical measurements in centimeters (cm) or millimeters (mm).
Small (Less than 1 cm to 5 cm):
1 cm: Size of a pea or seed.
3 cm: Size of a cherry or grape.
5 cm: Size of a lime.
Medium (5 cm to 10 cm):
7 cm: Size of a peach.
10 cm: Size of a grapefruit or an orange.
Large (10 cm and above):
15 cm +: Can resemble a melon or watermelon.
Large Fibroids Exceed the capacity of the pelvic cavity, often pushing against other organs like the bladder or rectum. If your doctor mentions your fibroid is the size of a grapefruit, it is generally considered significant and likely requires attention, especially if you have symptoms.
When Does Fibroid Size Become Dangerous?
A common question we hear is, “Is my fibroid dangerous?” It is important to know that fibroids are almost always benign (non-cancerous). However, “dangerous” in this context usually refers to complications or severe impact on health.
Which Size of Fibroid Is Dangerous in mm and cm?
There is no specific millimeter count that signals immediate danger. However:
Over 50 mm (5 cm): This is often the threshold where doctors start discussing treatment options if symptoms exist.
Over 100 mm (10 cm): These are considered giant fibroids. They can cause heavy bleeding, anemia, and compression of the ureters (kidney tubes), which is a medical urgency.
Impact on Surrounding Organs
As fibroid size increases, the uterus expands. A uterus the size of a 5-month pregnancy (due to fibroids) can press on the bladder, causing frequent urination, or the bowel, causing constipation. This physical bulk can disrupt normal activity, making exercise or even bending over uncomfortable.
Symptoms vs. Size: What Should You Worry About?
While we focus on average uterine fibroid size ranges, the severity of symptoms often dictates the treatment plan more than the ruler measurement.
You could have a massive 10 cm fibroid that grows outward and feel nothing. Conversely, a tiny 2 cm submucosal fibroid can cause:
Prolonged, heavy menstrual bleeding.
Passing large clots.
Severe pelvic pain and cramping.
Anemia and fatigue.
Therefore, do not just ask “how big is it?” but ask “how is it affecting my health?” If your normal activity is disrupted—you can’t go to work, you’re tired all the time, or you’re in pain—size becomes secondary to the need for relief.
How Fibroids Affect Pregnancy and Fertility
Which size of fibroid is dangerous in pregnancy?
Fibroids can affect fertility and pregnancy, but many women with fibroids have healthy babies.
Location matters: Fibroids inside the cavity (submucosal) can prevent implantation, acting like a natural IUD.
Size matters: Large fibroids (>5-6 cm) may compete for space with the baby or cause placental abruption.
Growth: Pregnancy hormones can cause fibroids to grow rapidly in the first trimester.
If you are planning to conceive, it is crucial to talk to a specialist like Dr. Samir. Treating the fibroid before pregnancy using uterine artery embolization (catheterization) or other methods might be recommended depending on your specific case.
Menopause and the Changing Uterus
Which size of fibroid is dangerous after menopause?
Typically, fibroid symptoms subside after menopause because hormone levels drop, causing the tumors to shrink. However, if a fibroid begins to grow after menopause, this is a red flag.
While rare, rapid growth after menopause can indicate a leiomyosarcoma (cancer). Therefore, any change in fibroid normal size post-menopause requires immediate investigation. A fibroid should not be getting bigger when you are no longer menstruating.
Diagnostic Methods: Measuring the Mass
To determine the exact size of the fibroids, a simple pelvic exam isn’t enough.
Ultrasound: The first step. It gives a good estimate of size in centimeters.
MRI (Magnetic Resonance Imaging): The gold standard. It maps the exact location, number, and size of fibroids and distinguishes them from adenomyosis.
Dr. Samir Abdel Ghaffar utilizes precise imaging to plan the Interventional Radiology procedure. By seeing exactly which arteries are feeding the tumors, he can target them effectively irrespective of their size.
The Risks of Leaving Large Fibroids Untreated
Choosing to leave a fibroid untreated (Watchful Waiting) is a valid option for Smaller fibroids with no symptoms. However, ignoring growing or symptomatic fibroids carries risks:
Severe Anemia: From chronic blood loss.
Kidney Damage: If a large fibroid presses on the ureter.
Infertility: As discussed, they can distort the uterus.
Lifestyle Deterioration: Living with constant pain or bloating.
Why Catheterization (UFE) is the Best Alternative to Surgery
For years, the only answer to “it’s too big” was “let’s take it out” (Hysterectomy or Myomectomy). Today, you have options.
Uterine Fibroid Embolization (UFE), performed by Interventional Radiology Consultants like Dr. Samir Abdel Ghaffar, is a revolutionary procedure.
No Surgery: No scalpels, no large incisions.
Preserves the Uterus: You keep your organs.
Shrinks Fibroids: The doctor inserts a tiny catheter into the artery ensuring blood flow to the fibroid is cut off. The fibroid then shrinks and dies.
Short Recovery: Return to normal activity much faster than surgery.
Whether your fibroid is the size of a grapefruit or a lime, UFE is effective for multiple fibroids simultaneously.
Frequently Asked Questions (FAQs)
Here, we answer the specific questions you might have about your diagnosis.
Size of fibroid in cm and mm?
Doctors may use both units. 1 cm = 10 mm.
Small: < 5 cm (< 50 mm)
Medium: 5–10 cm (50–100 mm)
Large: > 10 cm (> 100 mm)
Which size of fibroid is dangerous in mm?
There is no dangerous “number,” but fibroids exceeding 50 mm often start causing symptoms. Fibroids larger than 150 mm (15 cm) are significantly large and can mimic a 6-month pregnancy.
Is a 30 mm fibroid big?
No, a 30 mm (3 cm) fibroid is considered small (roughly the size of a strawberry). Unless it is located inside the uterine cavity causing bleeding, it is usually not a cause for alarm.
Is a 4 cm fibroid big?
A 4 cm fibroid is small to medium (size of a walnut or fig). It is very common. Many women have 4 cm fibroids and don’t even know it. However, if it pushes on your bladder, it might feel bigger than it is!
Can fibroids cause coughing?
Rarely, yes. If Large Fibroids Exceed the pelvic brim and grow large enough to press against the diaphragm or lungs, they can restrict breathing or cause a reflex cough. This is a sign of a very large fibroid requiring treatment.
What size fibroids should I worry about?
You should worry about any size that causes:
Heavy periods soaking through pads in an hour.
Pelvic pressure that hurts.
Trouble emptying your bladder.
Rapid growth (e.g., doubling in size in 6 months).
Fibroid sizes chart?
(Refer to the “From Seed to Watermelon” section above). Keeping a personal chart of your ultrasound results year over year is a good way to track growth.
Conclusion: Take Control of Your Uterine Health
Knowing which size of fibroid is normal is the first step toward empowerment. Whether your fibroids are small seeds or have grown to the size of a grapefruit, you do not have to suffer in silence or rush into removing your uterus.
Dr. Samir Abdel Ghaffar offers a safe, effective, and non-surgical path to reclaiming your life. Uterine Fibroid Embolization treats the root cause, shrinking the fibroids and alleviating symptoms while allowing you to keep your uterus intact. 🌿
Don’t let the numbers on a page scare you. Seek a consultation today to explore if UFE is right for you.
Do heavy periods and pelvic pain control your daily life, making you feel trapped by your own body? The fear of major surgery or losing your uterus often prevents women from seeking help, leaving them suffering in silence.
But you don’t have to choose between living in pain and undergoing a hysterectomy. Today, advanced medical science offers a safe, effective solution through the treatment of fibroids without surgery, restoring your health and peace of mind.
Is Fibroid Curable Without Surgery?
Many women diagnosed with uterine fibroids immediately fear that the only “cure” is a hysterectomy (removal of the uterus). This is a common misconception that has led countless women to undergo unnecessary major surgeries. The short answer is: Yes, the symptoms and the impact of the disease can be effectively “cured” or managed without removing the organ.
While “cure” in a strict medical sense often implies the complete eradication of every single cell, the goal of modern Fibroid Care is to eliminate the problems the fibroids cause—pain, bleeding, and bulk symptoms—and to shrink the tumors significantly so they no longer affect your life.
Non-surgical fibroid treatments focus on targeting the fibroid tissue itself while leaving the healthy uterus intact. Approaches like Uterine Fibroid Embolization (UFE) have revolutionized how we approach these benign growths. By cutting off the blood supply to the fibroids, we cause them to shrink and die. The body then naturally absorbs the treated tissue over time.
This approach is particularly vital for women of reproductive age who wish to preserve their uterus, or for those who simply want to avoid the long recovery times and risks associated with invasive surgery. Studies and data from major institutions like the Mayo Clinic have highlighted the efficacy of these minimally invasive techniques in providing lasting relief.
New Treatment for Fibroids Without Surgery: The UFE Revolution
When we discuss the new treatment of fibroids without surgery, we are primarily talking about the advancements in Interventional Radiology, specifically Uterine Fibroid Embolization (UFE). This is the cornerstone of Dr. Samir Abdel Ghaffar’s practice.
What is UFE?
Unlike a myomectomy (surgical removal of fibroids) or hysterectomy, UFE does not require general anesthesia or large incisions. It is a minimally invasive procedure performed through a tiny pinhole in the wrist or groin.
How does it work?
Catheterization: Dr. Samir inserts a very thin catheter into the blood vessels.
Navigation: Using advanced imaging (fluoroscopy), he guides the catheter to the uterine arteries that supply blood to the fibroids.
Embolization: Tiny particles (microspheres) are injected to block these specific vessels.
Result: Deprived of blood and nutrients, the fibroids begin to shrink immediately. The symptoms—heavy bleeding, pain, and pressure—often improve dramatically within the first cycle after the procedure.
This method is considered one of the most effective ways to treat multiple fibroids at once, regardless of their location or number. It is an expert approach that treats the entire uterus in one session, reducing the percentage of recurrence compared to removing individual fibroids surgically.
Best Treatment for Large Fibroids
A common question patients ask Dr. Samir is, “My doctor said my fibroids are too big for anything but surgery. Is that true?”
In the past, size was a limiting factor for non-surgical options. However, with the advanced techniques used in UFE, size is rarely a barrier. In fact, UFE is often the best treatment options for large or multiple fibroids because it avoids the massive trauma a surgeon would have to inflict on the uterus to cut them out.
When you surgically remove a large fibroid, you risk significant blood loss and the formation of scar tissue (adhesions), which can cause future pain or fertility issues. Nonsurgical treatment options like embolization treat the fibroid from the “inside out.” Even very large fibroids can shrink by 50-60% in volume, which is usually enough to stop them from pressing on the bladder or bowel and to flatten the abdomen.
Benefits of UFE for Large Fibroids:
No abdominal scar: The procedure is internal.
Shorter recovery: You can typically return to normal life in days, not weeks.
Safety: It avoids the risks of major surgery, such as infection or injury to other organs.
How to Shrink Fibroids Naturally Without Surgery
Many women prefer to explore natural avenues before committing to a medical procedure. While lifestyle changes cannot typically “cure” existing large fibroids or make them vanish, they play a crucial role in managing symptoms, preventing further growth, and supporting health after a procedure like UFE.
Hormonal Balance and Lifestyle
Fibroids are hormonally driven, thriving on estrogen. Therefore, a lifestyle that promotes hormonal balance can be helpful. This includes managing stress, getting enough sleep, and avoiding exposure to xenoestrogens (chemicals that mimic estrogen) found in certain plastics and pesticides.
Weight Management
Fat cells produce estrogen. Maintaining a healthy weight through diet and exercise can help regulate the hormone levels in your body, potentially slowing fibroid growth.
7 Foods for Shrinking Fibroids
While no single food is a “magic bullet,” an anti-inflammatory diet can help relieve symptoms and create an environment less improved for tumor growth. Here are 7 dietary additions to consider:
Cruciferous Vegetables: Broccoli, cauliflower, and kale contain indole-3-carbinol, which supports the liver in metabolizing excess estrogen.
Green Tea: Contains EGCG, an antioxidant shown in some studies to inhibit fibroid cell growth.
Citrus Fruits: Rich in Vitamin C and bioflavonoids, which help strengthen blood vessels and may reduce heavy bleeding.
Flaxseeds: High in fiber and lignans, helping the body eliminate excess estrogen safely.
Fatty Fish: Salmon and mackerel are rich in Omega-3 fatty acids, which reduce inflammation and painful cramping.
Berries: Blueberries and strawberries are packed with antioxidants that fight oxidative stress.
Vitamin D-Rich Foods: There is a strong link between Vitamin D deficiency and fibroid formation. Fortified foods or safe sun exposure are key.
Note: Always discuss dietary changes with your doctor, especially if you are taking medications.
Fibroid Removal Without Surgery Cost
Cost is a practical and important consideration. When comparing the Treatment of Fibroids Without Surgery (UFE) to traditional surgery, there are several factors to keep in mind.
While we do not list specific prices here as they vary by case and insurance coverage, UFE is generally cost-effective when you consider the “total cost” of recovery.
Hospital Stay: Surgery often requires 2-4 days in the hospital. UFE is typically a day-case or requires only an overnight stay.
Return to Work: Recovery from a hysterectomy can take 6 to 8 weeks. UFE patients often return to work within a week. This means less lost income and better productivity.
Medication and Aftercare: The need for long-term pain medication and wound care is significantly lower with non-surgical options.
Dr. Samir’s team works with various medical insurance providers to ensure this safe treatment is accessible.
New Treatment for Fibroids Surgery
It is fair to ask: “What if I do need surgery?” While this article focuses on avoiding it, it is important to understand the landscape.
Newer surgical methods, like robotic-assisted myomectomy, are less invasive than open surgery but still carry surgical risks. They involve anesthesia, incisions, and uterine scarring. The distinct advantage of Dr. Samir’s approach—uterine fibroid embolization—is that it is completely nonsurgical.
There is also a technology called Focused Ultrasound Surgery (FUS or HIFU), which uses sound waves to heat and destroy fibroid tissue inside an MRI machine. While promising, it is time-consuming and often not suitable for women with multiple or very large fibroids. UFE remains the most versatile non-surgical option that covers the widest range of patient conditions.
Frequently Asked Questions
To help you learn more and make an informed decision, here are answers to common questions we receive at the clinic.
Can fibroids cause fever?
Generally, fibroids do not cause fever. However, if a fibroid grows very rapidly and outgrows its blood supply, it can degenerate (break down), causing pain and a low-grade fever. If you have fibroids and experience a high fever, it is crucial to see a doctor immediately to rule out infection or other common complications.
When to remove fibroids in the uterus?
“Removal” isn’t always necessary. You should seek treatment (whether UFE or removal) if the fibroids are causing symptoms that affect your quality of life—such as heavy periods, anemia, severe pelvic pain, or bladder pressure. If fibroids are small and asymptomatic, “watchful waiting” with regular ultrasound monitoring is often recommended.
Can fibroids cause Nausea?
Yes, large fibroids can press on the stomach or intestines, leading to digestive issues, bloating, and a sensation of nausea, especially after eating.
Can fibroids cause shortness of breath?
In rare cases involving extremely large fibroids, the uterus can expand upward into the abdominal cavity, pressing against the diaphragm. This restricts lung expansion and can cause shortness of breath or difficulty breathing deeply. This is a sign that immediate intervention is needed.
Why Choose Dr. Samir Abdel Ghaffar?
Your health is your most valuable asset. Dr. Samir Abdel Ghaffar is a renowned Consultant in Interventional Radiology, specializing in the treatment of fibroids without surgery. With years of experience in both the UK and Egypt, he offers a level of care that prioritizes organ preservation and patient comfort.
Dr. Samir utilizes the latest catheterization techniques to ensure the procedure is painless and effectively targets the tumors. His approach is holistic, understanding that every woman’s body and goals are different.
By choosing uterine artery embolization, you are choosing a faster recovery, no surgical scars, and the preservation of your uterus. It is a safe, modern alternative that has helped thousands of women regain their lives 🌟.
If you are suffering from fibroids and want to avoid the risks of major surgery, contact us today to discuss if you are a candidate for this life-changing procedure.
Do you dread your monthly cycle because of excruciating cramps and bleeding that keeps you bedridden? You might be suffering from a condition affecting your uterus, yet unsure of the cause. Understanding the distinction between Adenomyosis vs. Uterine Fibroids is the first step toward reclaiming your life without losing your uterus.
What Is the Main Difference Between Adenomyosis vs. Uterine Fibroids?
The confusion is understandable. Both conditions affect the uterus, cause heavy bleeding, and can make life miserable for women. However, they are biologically distinct.
The main difference lies in where the growth occurs. Uterine Fibroids are benign tumors that grow on or in the muscular wall of the uterus. They are solid masses of tissue. Think of them like knots or stones growing within the muscle.
On the other hand, Uterine adenomyosis is not a tumor. It occurs when the endometrial tissue (the lining of the uterus that you shed during your period) breaks through and grows into the muscle tissue of the uterus. It’s like the lining is invading the muscle wall, causing the uterus to become boggy, bulky, and painful. While fibroids are distinct lumps, adenomyosis is more of a diffuse condition affecting the muscle structure itself.
Understanding Uterine Fibroids: The Benign Growths
Uterine fibroids are the most common benign tumors of the female reproductive system. They can vary wildly in size—from a tiny seed to a melon.
Fibroids are essentially overgrowths of smooth muscle cells and connective tissue. They are almost always non-cancerous. You might have one single fibroid or multiple clusters. They are categorized by their location:
Subserosal: On the outside wall.
Intramural: Within the muscular wall.
Submucosal: Bulging into the uterine cavity.
While the majority of women will develop fibroids at some point, not everyone has symptoms. But when they do grow large, they cause pressure, bulk symptoms, and heavy menstrual bleeding.
Understanding Adenomyosis: The Internal Invasion
Adenomyosis is often called the sister of endometriosis, but they are different. In endometriosis, the lining grows outside the uterus. In adenomyosis, it grows inside the myometrium (the muscle wall).
When you have your period, this trapped endometrial tissue inside the muscle tries to bleed just like the lining in the cavity. But because it’s trapped inside the muscle, it causes tiny pools of blood, inflammation, and severe cramping as the muscle stretches and contracts.
This condition typically results in a uniformly enlarged uterus. If you’ve been told your uterus looks bulky or globular, it might be adenomyosis.
Shared Symptoms: Why Confusion Occurs
Why is it so hard to tell them apart without imaging? Because fibroids and adenomyosis share remarkably similar symptoms. Both are the most common causes of abnormal uterus bleeding and pelvic pain.
Common overlap includes:
Heavy and prolonged menstrual periods.
Severe menstrual cramping (Dysmenorrhea).
Abdominal bloating or pelvic pressure.
Pain during intercourse.
Anemia due to blood loss.
Because of these overlaps, many women are misdiagnosed or simply told they have fibroids when they might actually have adenomyosis, or even both conditions simultaneously.
How to Accurately Diagnose the Conditions
A simple pelvic exam isn’t enough to distinguish between the two. Your doctor needs to look under the hood.
Ultrasound: This is the first step. Uterine Fibroids are usually easy to spot on an ultrasound as distinct, round masses with defined borders. Adenomyosis is more subtle; it appears as a heterogenous (uneven) texture in the muscle wall, often with venetian blind shadowing or an enlarged wall on one side.
MRI (Magnetic Resonance Imaging): This is the gold standard. An MRI can accurately map the location of fibroids and clearly show the thickening of the junctional zone, which is the hallmark of adenomyosis. This precision is crucial for planning treatment, especially for interventional radiology.
Risk Factors: Who Gets Them?
While the exact cause is unknown for both, hormones play a huge role. Estrogen drives the growth of both fibroids and adenomyosis, which is why symptoms often resolve after menopause.
Fibroids: More common in women of African descent, those with a family history, and women who have never been pregnant.
Adenomyosis: Often seen in women who have had children (specifically C-sections or uterine surgeries) and typically presents later in the reproductive years (40s and 50s), though it affects younger women too.
Can You Have Both Conditions Together?
Yes, and it is actually quite common. Many women are diagnosed with fibroids because they are easy to see, while the underlying adenomyosis is missed.
Having both can exacerbate symptoms, leading to even heavier bleeding and more severe pain. This makes accurate diagnosis vital. If a doctor only removes the fibroids (myomectomy) but leaves the adenomyosis untreated, the painful symptoms will likely continue.
Impact on Fertility and Pregnancy
Both conditions can affect your ability to get pregnant or maintain a pregnancy, but in different ways.
Fibroids: Depending on their location (especially if they are inside the cavity), they can prevent implantation or cause miscarriage.
Adenomyosis: The chronic inflammation in the uterine wall can make implantation difficult and may increase the risk of early miscarriage.
However, many women with these conditions go on to have healthy babies. It depends on the severity. It is crucial to discuss your fertility goals with Dr. Samir, as some treatments are better suited for women who wish to conceive than others.
Non-Surgical Treatment: The Catheterization Revolution
For decades, the standard cure for adenomyosis was a hysterectomy (removing the uterus). For fibroids, it was either myomectomy or hysterectomy.
Dr. Samir Abdel Ghaffar offers a safe, modern alternative: Uterine Artery Embolization (UAE), also known as Uterine Fibroid Embolization (UFE).
How it works for both:
The procedure involves inserting a tiny catheter (a thin tube) through a blood vessel in the leg or wrist. Guided by real-time imaging, Dr. Samir directs the catheter to the uterine arteries. He then injects tiny particles (microspheres) to block the blood supply.
For Fibroids: Deprived of blood, the fibroids shrink and die.
For Adenomyosis: The particles block the blood flow to the abnormal tissue in the muscle wall, causing it to shrink and the symptoms to improve significantly.
Why Choose Embolization Over Surgery?
The benefits of choosing catheterization (Interventional Radiology) are significant, especially for women who want to avoid major surgery.
Preserves the Uterus: You do not have to lose your organ to lose the pain.
Short Recovery: Most patients go home the same day or the next morning and return to normal activity within a week.
Treats Both: Embolization is unique because it treats fibroids and adenomyosis simultaneously. You don’t need to surgically remove every single fibroid; the embolization targets the entire uterus’s blood supply in a controlled way.
No Scars: No abdominal incision.
Lifestyle Changes to Help Manage Symptoms
While medical treatment is often necessary, certain lifestyle adjustments can help manage flare-ups:
Anti-inflammatory Diet: Reducing red meat, gluten, and sugar can lower overall inflammation.
Heat Therapy: Heating pads can relax the uterine muscles.
Supplements: Magnesium and Omega-3s may help reduce cramping severity.
However, these are supportive measures. They do not remove the tumors or the adenomyosis tissue.
Conclusion: You Don’t Have to Live in Pain
Whether it is the distinct lump of a fibroid or the diffuse pain of adenomyosis, you deserve relief. Understanding the Adenomyosis vs. Uterine Fibroids distinction ensures you get the right treatment.
Dr. Samir Abdel Ghaffar specializes in treating both conditions using advanced interventional radiology. By blocking the blood supply to these benign growths, he helps you improve your quality of life without the risks and downtime of surgery. 🌿
Don’t let pelvic pain dictate your life. Discover your options today.
Frequently Asked Questions (FAQs)
How to differentiate between fibroids and adenomyosis?
The only way to be 100% sure is through imaging. An ultrasound can often see fibroids, but an MRI is the best tool to distinguish the diffuse thickening of the uterine wall (adenomyosis) from the solid round masses (fibroids).
Can adenomyosis be misdiagnosed as fibroids?
Yes, frequently. Because fibroids are more famous and easier to see on basic ultrasounds, doctors often blame the symptoms on a small fibroid while missing the adenomyosis hiding in the muscle wall.
Can adenomyosis cause headaches?
Adenomyosis itself doesn’t directly cause headaches. However, the severe anemia resulting from heavy bleeding can cause headaches, dizziness, and fatigue. Also, the hormonal imbalances driving the condition can trigger migraines.
Can fibroids cause nausea?
Yes. If a fibroid is very large, it can press on the stomach or intestines, leading to feelings of fullness, bloating, and nausea. Intense pain from degenerating fibroids can also cause nausea.